
Critical Care
The Southwest Journal of Pulmonary and Critical Care publishes articles directed to those who treat patients in the ICU, CCU and SICU including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.

October 2024 Critical Care Case of the Month: Respiratory Failure in a Patient with Ulcerative Colitis
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
The patient is a 57-year-old woman with a history of ulcerative colitis (UC) complicated by toxic megacolon with subsequent colectomy. She presented to the emergency department with cough, shortness of breath and hypoxemia (87% on RA).
PMH, SH
- UC with history of toxic megacolon (4 years prior) with a total colectomy.
- History of a prior episode of respiratory failure a year earlier thought possibly medication-induced (ustekinumab, Stelara®) which she was taking for her UC. She was treated with steroids with a good response.
- Pyoderma gangrenosum of both ankles (attributed to UC).
- Anemia of chronic disease.
- She is a lifelong non-smoker.
- No exposures to toxic dusts, birds, down, humidifiers, mold or other antigens associated with hypersensitivity pneumonitis.
Physical Exam
- Afebrile, Oxygen saturation 94% on 2 lpm supplemental oxygen.
- Chest: crackles noted at left base.
- CV regular rhythm, no murmur.
- Ext: scarring and erythema on both ankles consistent with resolving pyoderma gangrenosum.
Current Medications
- Clonazepam 1.0 mg daily at bedtime
- Gabapentin 300 mg TID
- Pantoprazole 40 mg BID
- Prednisone 5 mg daily
Laboratory
- Hgb 9.7, WBC 16.9
- Swabs for Influenza A/B and Covid were negative
- Cocci serology negative
A chest radiograph was performed (Figure 1).
 Figure 1. Portable chest X-ray performed in the emergency department. (To view Figure 1 in a separate, enlarged window click here).
Figure 1. Portable chest X-ray performed in the emergency department. (To view Figure 1 in a separate, enlarged window click here).
{kind=link}
Which of the following is/are true regarding the chest X-ray?
- There is a left lower lobe consolidation.
- The portable chest X-ray may be normal.
- A chest CT scan is required to definitely view any consolidation.
- There is a right upper lobe consolidation.
- All of the above.
The Effect of Low Dose Dexamethasone on the Reduction of Hypoxaemia and Fat Embolism Syndrome After Long Bone Fractures
Dr. Akash K
Dr. Madhuchandra R
Department Of Orthopaedics, Karnataka Institute Of Medical Sciences, Hubli, India
Abstract
Background: A dangerous and sometimes fatal consequence of post-traumatic long bone fractures is fat embolism syndrome (FES). The reported incidence of FES ranges from 2% to 22%. FES can also lead to critical illness with fatality rates between 10 to 36%. This study's objective was to determine whether prophylaxis of the fat emboli syndrome could be achieved with lower doses of dexamethasone than had previously been recommended. Thus, prevention of respiratory insufficiency and disruption of homeostasis are essential.
Methods: A total of 583 adult cases of long bone shaft fracture patients between January 2020 to December 2021 were randomly divided into a trial group (n= 252) and a control group (n=331) by simple randomization. The trial group received dexamethasone 8mg/day for 3 days and the control group was given placebo. FES was diagnosed using Gurd’s diagnostic criteria and the FES morbidity and death rates in each group were examined.
Results: Five patients (0.151%) in the control group and 1 patient (0.39%) in the trial group developed FES but the difference was not significant (p>0.05). SpO2 values were significantly elevated in the dexamethasone-treated group compared to the control group 24 hours after admission (p<0.05) and the elevation persisted on the third post admission day (p<0.05).
Conclusion: Dexamethasone in low doses reduces post-traumatic hypoxia in patients with long bone fracture. However, our study was underpowered to show a reduction in FES.
Introduction
Fat emboli occur in all long bone fractures with the most severe resulting in fat embolism syndrome (FES). The reported incidence of FES ranges from 2% to 22% with fatality rates of 10-36% (1-3) with FES resulting in the adult respiratory distress syndrome a 50–90% mortality rate (1-3). Unfortunately, this is particularly common in young people in their second and third decades of life who sustain polytrauma and/or femur fractures in high-velocity traffic accidents (2,3). The majority of trauma patients may experience a subclinical form of FES, which manifests as hypoxaemia alone (3-6).
FES resulting in systemic symptoms is a rare clinical outcome. Following a traumatic incident, fat droplets are released into the bloodstream resulting in fat embolization. This results in immediate tissue damage as well as a systemic inflammatory response that produces symptoms in the lungs, skin, nervous system, and retina (7,8). Most instances of FES occur after trauma but rare cases of FES have been reported to occur after bone marrow transplantation, osteomyelitis, pancreatitis, alcoholic fatty liver, and even liposuction (9,10). Although the classic triad of pulmonary distress, mental status changes, and petechial rash is usually not seen, hypoxia 24 to 48 hours after pelvic or long-bone fractures is common (11-13).
FES has no pathognomonic characteristics and laboratory and radiographic findings are nonspecific (14,15). Early detection of FES may allow supportive pulmonary treatment and other life-saving interventions to stop the pathophysiologic cascade and stop clinical deterioration. The majority of curative methods created expressly for FES have failed (16,17). There have been several attempts to avoid FES since it is such a serious issue in trauma patients (4). With varying degrees of success, heparin, dextran, albumin, hypertonic glucose, aspirin, and early fracture stabilization, have all been attempted (4). Steroids have also been studied as a preventative as well as a therapeutic agent in fat embolism in various studies.
When fat droplets act as emboli and are trapped in the pulmonary microvasculature and other microvascular beds, such as the brain, they may cause clinical symptoms to appear 24-72 hours after trauma (and particularly after fractures). Embolization starts out very slowly and reaches its peak in 48 hours or more. A long-acting corticosteroid having a half-life of 36 to 72 hours is dexamethasone. This study's objective was to determine whether prophylaxis of the fat emboli syndrome could be achieved with lower doses of dexamethasone than had previously been recommended (17).
Patients and Methods
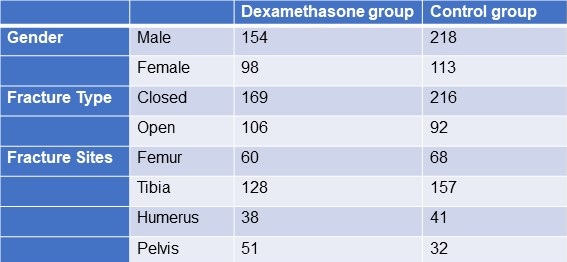
From January 2020 to December 2021, 583 adult patients between the ages of 18 and 60 with long bone fractures without a history of chronic heart, lung, liver, or renal failure were recruited from patients at KIMS Hospital Hubli. There were 211 cases observed in women and 372 cases in men. The injuries resulted from motor accidents (426), falls (127), and crush injuries (30). Fracture sites included 128 femur fractures, 285 tibia and fibula fractures, 79 humerus fractures, and 91 pelvic injuries. The patients were randomized into two groups, one receiving dexamethasone and the other receiving a placebo (Table 1).
Table 1. Demographic data

Click here to display Table 1 in a separate, enlarged window.
{kind=link}
The following patient information was recorded: gender, age, weight, time from injury to admission, primary fracture location, type of fracture, FES morbidity, and number of fatalities. All patients received traditional medical care, early hypovolemic shock correction, fracture stabilization, and symptomatic therapy (2). The trial group received dexamethasone 8mg/day for 3 days and the control group was given placebo. All patients were monitored (heart rate, BP, SpO2 ,respiratory rate, urine output, and arterial blood gases) every 6 hours for 3 days. We considered hypoxaemia with any pO2 <70mm Hg and classified all patients in 3 categories; severe (pO2<60mm Hg), mild hypoxaemia (pO2 >60- <70 mm Hg) and normal (pO2>70mm Hg). All patients signed an informed consent form. The study was approved by the Ethics Committee of our institute hospital.
Treatment and diagnosis for FES
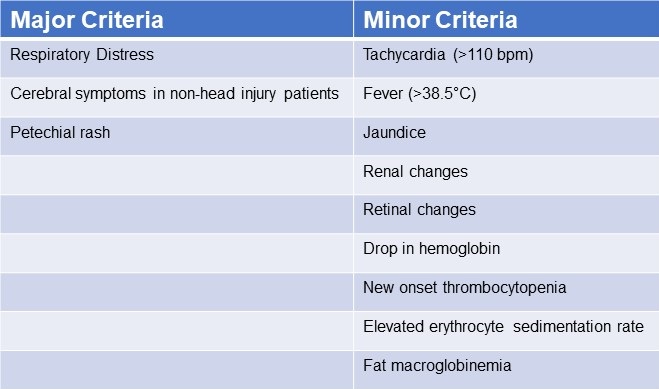
Patients were identified using “Gurd’s Diagnostic criteria score”(Table 2), and those whose score was 2 major or 1 major and 4 minor were diagnosis as FES.
Table 2. Gurd’s Diagnostic Criteria Score*

*Two major criteria or 1 major criterion and 4 minor criteria suggest a diagnosis of FES. Click here to view Table 2 in a separate and enlarged window.
{kind=link}
Data analysis
Utilizing statistical tools, the analysis was conducted (SPSS 20.0). P< 0.05 was regarded as statistically significant when comparing the patients' age, main fracture location, fracture type, and incidence of FES using the chi-squared test and single-factor analysis of variance, respectively.
Results
FES occurred in the dexamethasone group and control group, with 1 and 5 cases, respectively (Table 3). Statistical analysis revealed that there was no statistically significant difference between the groups for sex, age, weight, injury to admission time, main fracture site, fracture type, or medication time.
Table 3. Incidence of FES
 Click here to view Table 3 in a separate, enlarged window.
Click here to view Table 3 in a separate, enlarged window.
{kind=link}
Twenty-four hours after admission, steroid treated patients displayed a statistically significant higher PaO2 value compared to the control group (p<0.05) and this difference persisted through the 3rd post admission day (p<0.05, table 4).
Table 4. Partial pressures of oxygen (in mm Hg) in patients treated with IV dexamethasone and controls.

Click here to view Table 4 in a separate and enlarged window.
{kind=link}
Discussion
Much higher dosages of dexamethasone have been used to treat some pathological conditions in order to reduce inflammation, inhibit the immune system, impact the hemopoietic system, and alter metabolism (18-28). The mechanical-chemical hypothesis of fat embolism hypothesizes that neutral triglycerides are hydrolyzed into glycerol and free fatty acids by lipoprotein lipase from the lungs. The free fatty acids lead to inflammation and endothelial damage. Corticosteroids likely act on FES by reducing this inflammation. Due to a lack of clear diagnostic markers, treating FES may prove challenging. There have been few publications on the use of adrenal steroids to prevent high-risk FES patients, although the results have been ambiguous at low doses (31). Observational clinical research revealed that short-range and high doses may be helpful in reducing plasma free fatty acid concentrations, maintaining PaO2 levels, and reducing the occurrence of long bone fractures in individuals with FES. Dexamethasone may be a more effective drug treatment for FES (32). The dose of dexamethasone used in our study was relatively small and short, and complications related to hormones such as stress ulcer, aseptic necrosis of the femoral head, and bleeding tendency did not occur. It should be noted that drug prevention must be based on early, accurate fracture fixation, early corrective hypovolemic shock, and other standard procedures (33). This is true even if drug usage in this population clearly has a preventative impact. Ashbaugh and Petty (34) suggested corticosteroid therapy for treating FES in 1966 and gave laboratory data proving its therapeutic impact in the experimental animal given an intravenously administered FFA injection. Rokkanen et al. (35) found that 5 mg/kg of dexamethasone administered at 1 and 48 h after burn injury failed to enhance nuclear translocation of the GR, and to suppress the overproduction of proinflammatory cytokines such as TNF-α and IL-1β, neither did it increase the release of anti-inflammatory cytokine IL-10. In experiments with animals, Kreis et al. (36) showed that corticosteroids increased oxygenation and lowered the pathological alterations seen in lung biopsies. Alho et al. (37) conducted research on the use of intravenous methyl prednisolone sodium succinate in the prevention of fat embolism syndrome. A total of 60 individuals with at least two fractures were included in his study (pelvic, femoral or tibial fractures).methyl prednisolone reduces signs of hypoxaemia, bilateral "snow storm" infiltrations of the lungs, petechial rash, mental disturbances, pyrexia, anemia and thrombocytopenia. Varying degrees of the syndrome were observed in two patients given methylprednisolone and in 15 patients in the control group. Babalis et al. (39) results support the prophylactic administration of methylprednisolone in small dosage to prevent post traumatic hypoxaemia and probably FES in patients with isolated lower limb long bone fractures, especially when early fracture stabilization is not possible. Therefore, every study has demonstrated the effectiveness of steroids as a preventative treatment for the fat embolism syndrome.
Although our results showed a trend towards reduction in FES after long bone fractures, the results were not statistically significant. This is likely because our study turned out to be underpowered. We had anticipated an incidence of FES between 2-20% reported in the literature rather than the 1.1% found in our study.
Conclusion
The study's objective was to determine whether prophylaxis of the fat emboli syndrome could be achieved with lower doses of dexamethasone than had previously been recommended. Among the several prophylactic drugs that have been researched so far for the fat embolism syndrome, dexamethasone have shown to be relatively beneficial. The frequency of hypoxaemia and fat emboli syndrome decreased with intravenous dexamethasone at 8 mg per day for three days. Dexamethasone is a long-acting symptoms that emerge 24-72 hours after trauma (and particularly after fractures). Fat embolization begins slowly and reaches its maximum around 48 hours.
The limitation of our study is that it lacked sufficient power to demonstrate a reduction in FES. Furthermore, no method has been developed to pinpoint precisely who could benefit from steroid prophylaxis. We based our study assuming an incidence of FES of about 5%. However, we found an incidence of only about 1.5%. The lower incidence is probably due to our use of Gurd’s criteria which is more restrictive than the criteria used in other studies. Based on our observed incidence of FES of 1.5% with a reduction to 0.4% we estimate that over 2500 patients would be needed to show a statistically significant reduction in FES.
Our study shows that hypoxaemia is reduced by a relatively low dose of dexamethasone administered for a relatively short length of time. It may prevent FES but our study was underpowered to show a difference.
Declaration
Human subjects: Consent was obtained or waived by all participants in this study. Karnataka Institute Of Medical Sciences ethics committee. issued approval 327/2020-21. The study was approved by the institutional ethics committee. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissues. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all
authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work
References
- Sproule BJ. Brady JL. Gilbert J. Studies on the Syndrome of Fat Embolization. Can Med Assoc J. 1964 May 30;90(22):1243-7. [PubMed]
- Wertzberger JL, Peltier LF. Fat embolism: the importance of arterial hypoxia. Surgery. 1968 Apr;63(4):626-9. [PubMed]
- Stürm JA, Lewis FR Jr, Trentz O, Oestern HJ, Hempelman G, Tscherne H. Cardiopulmonary parameters and prognosis after severe multiple trauma. J Trauma. 1979 May;19(5):305-18. [CrossRef] [PubMed]
- Hutchins PM, Macnicol MF. Pulmonary insufficiency after long bone fractures. Absence of circulating fat or significant immunodepression. J Bone Joint Surg Br. 1985 Nov;67(5):835-9. [CrossRef] [PubMed]
- Levy D. The fat embolism syndrome. A review. Clin Orthop Relat Res. 1990 Dec;(261):281-6. [PubMed]
- Gossling HR, Pellegrini VD Jr. Fat embolism syndrome: a review of the pathophysiology and physiological basis of treatment. Clin Orthop Relat Res. 1982 May;(165):68-82. [PubMed]
- Kwiatt ME, Seamon MJ. Fat embolism syndrome. Int J Crit Illn Inj Sci. 2013 Jan;3(1):64-8. [CrossRef] [PubMed]
- Parisi DM, Koval K, Egol K. Fat embolism syndrome. Am J Orthop (Belle Mead NJ). 2002 Sep;31(9):507-12. [PubMed]
- Scuderi CS. The present status of fat embolism. Bibliographic review. Int Surg Digest 1934; 18: 195-215.
- Gurd AR. Fat embolism: an aid to diagnosis. J Bone Joint Surg Br. 1970 Nov;52(4):732-7. [PubMed]
- Nixon JR, Brock-Utne JG. Free fatty acid and arterial oxygen changes following major injury: a correlation between hypoxaemia and increased free fatty acid levels. J Trauma. 1978 Jan;18(1):23-6. [CrossRef] [PubMed]
- Parker FB Jr, Wax SD, Kusajima K, Webb WR. Hemodynamic and pathological findings in experimental fat embolism. Arch Surg. 1974 Jan;108(1):70-4. [CrossRef] [PubMed]
- Nijsten MW, Hamer JP, ten Duis HJ, Posma JL. Fat embolism and patent foramen ovale. Lancet. 1989 Jun 3;1(8649):1271. [CrossRef] [PubMed]
- Vedrinne JM, Guillaume C, Gagnieu MC, Gratadour P, Fleuret C, Motin J. Bronchoalveolar lavage in trauma patients for diagnosis of fat embolism syndrome. Chest. 1992 Nov;102(5):1323-7. [CrossRef] [PubMed]
- White T, Petrisor BA, Bhandari M. Prevention of fat embolism syndrome. Injury. 2006 Oct;37 Suppl 4:S59-67. [CrossRef] [PubMed]
- Laterre PF, Wittebole X, Dhainaut JF. Anticoagulant therapy in acute lung injury. Crit Care Med. 2003 Apr;31(4 Suppl):S329-36. [CrossRef] [PubMed]
- Bederman SS, Bhandari M, McKee MD, Schemitsch EH. Do corticosteroids reduce the risk of fat embolism syndrome in patients with long-bone fractures? A meta-analysis. Can J Surg. 2009 Oct;52(5):386-93. [PubMed]
- McEvoy GK, Snow EK, Kester L, eds. AHFS 2002 Drug Information. Bethesda, MD: American Society of Health‐System Pharmacists; 2002.
- Chamberlain D. Emergency medical treatment of anaphylactic reactions. Project Team of the Resuscitation Council (UK). J Accid Emerg Med. 1999 Jul;16(4):243-7. [CrossRef] [PubMed]
- Niermeyer S, Kattwinkel J, Van Reempts P, et al. International Guidelines for Neonatal Resuscitation: An excerpt from the Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care: International Consensus on Science. Contributors and Reviewers for the Neonatal Resuscitation Guidelines. Pediatrics. 2000 Sep;106(3):E29. [CrossRef] [PubMed]
- Brun-Buisson C, Brochard L. Corticosteroid therapy in acute respiratory distress syndrome: better late than never? JAMA. 1998 Jul 8;280(2):182-3. [CrossRef] [PubMed]
- Hudson LD. New therapies for ARDS. Chest. 1995 Aug;108(2 Suppl):79S-91S. [CrossRef] [PubMed]
- Meduri GU, Headley AS, Golden E, Carson SJ, Umberger RA, Kelso T, Tolley EA. Effect of prolonged methylprednisolone therapy in unresolving acute respiratory distress syndrome: a randomized controlled trial. JAMA. 1998 Jul 8;280(2):159-65. [CrossRef] [PubMed]
- Johnson MJ, Lucas GL. Fat embolism syndrome. Orthopedics. 1996 Jan;19(1):41-8; discussion 48-9. [CrossRef] [PubMed]
- Kallenbach J, Lewis M, Zaltzman M, Feldman C, Orford A, Zwi S. 'Low-dose' corticosteroid prophylaxis against fat embolism. J Trauma. 1987 Oct;27(10):1173-6. [PubMed]
- Niewoehner DE, Erbland ML, Deupree RH, Collins D, Gross NJ, Light RW, Anderson P, Morgan NA. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med. 1999 Jun 24;340(25):1941-7. [CrossRef] [PubMed]
- Richards RR. Fat embolism syndrome. Can J Surg. 1997 Oct;40(5):334-9. [PubMed]
- Kubota T, Ebina T, Tonosaki M, Ishihara H, Matsuki A. Rapid improvement of respiratory symptoms associated with fat embolism by high-dose methylpredonisolone: a case report. J Anesth. 2003;17(3):186-9. [CrossRef] [PubMed]
- Han YY, Sun WZ. An evidence-based review on the use of corticosteroids in peri-operative and critical care. Acta Anaesthesiol Sin. 2002 Jun;40(2):71-9. [PubMed]
- Habashi NM, Andrews PL, Scalea TM. Therapeutic aspects of fat embolism syndrome. Injury. 2006 Oct;37 Suppl 4:S68-73. [CrossRef] [PubMed]
- Babalis GA, Yiannakopoulos CK, Karliaftis K, Antonogiannakis E. Prevention of posttraumatic hypoxaemia in isolated lower limb long bone fractures with a minimal prophylactic dose of corticosteroids. Injury. 2004 Mar;35(3):309-17. [CrossRef] [PubMed]
- Yamamoto T, Irisa T, Sugioka Y, Sueishi K. Effects of pulse methylprednisolone on bone and marrow tissues: corticosteroid-induced osteonecrosis in rabbits. Arthritis Rheum. 1997 Nov;40(11):2055-64. [CrossRef] [PubMed]
- Talbot M, Schemitsch EH. Fat embolism syndrome: history, definition, epidemiology. Injury. 2006 Oct;37 Suppl 4:S3-7. [CrossRef] [PubMed]
- Ashbaugh DG, Petty TL. The use of corticosteroids in the treatment of respiratory failure associated with massive fat embolism. Surg Gynecol Obstet. 1966 Sep;123(3):493-500. [PubMed]
- Rokkanen P, Alho A, Avikainen V, Karaharju E, Kataja J, Lahdensuu M, Lepistö P, Tervo T. The efficacy of corticosteroids in severe trauma. Surg Gynecol Obstet. 1974 Jan;138(1):69-73. [PubMed]
- Kreis WR, Lindenauer SM, Dent TL. Corticosteroids in experimental fat embolization. J Surg Res. 1973 Mar;14(3):238-46. [CrossRef] [PubMed]
- Alho A, Saikku K, Eerola P, Koskinen M, Hämäläinen M. Corticosteroids in patients with a high risk of fat embolism syndrome. Surg Gynecol Obstet. 1978 Sep;147(3):358-62. [PubMed]
- Stoltenberg JJ, Gustilo RB. The use of methylprednisolone and hypertonic glucose in the prophylaxis of fat embolism syndrome. Clin Orthop Relat Res. 1979 Sep;(143):211-21. [PubMed]
- Babalis GA, Yiannakopoulos CK, Karliaftis K, Antonogiannakis E. Prevention of posttraumatic hypoxaemia in isolated lower limb long bone fractures with a minimal prophylactic dose of corticosteroids. Injury. 2004 Mar;35(3):309-17. [CrossRef] [PubMed]
October 2020 Critical Care Case of the Month: Unexplained Encephalopathy Following Elective Plastic Surgery
Natalie Held, MD and Carolyn Welsh, MD
University of Colorado Division of Pulmonary Sciences and Critical Care Medicine
Aurora, CO USA
A 29-year-old woman with no significant medical history presents to the hospital due to progressive encephalopathy, 5 days after undergoing an elective abdominoplasty with abdominal liposuction and breast augmentation. She is somnolent on exam, and is hypoxic to ~60% saturation on room air. She is emergently intubated in the emergency department prior to being admitted to the MICU, and is started on broad-spectrum antibiotics and n-acetyl cysteine (NAC). She has evidence of acute liver failure but her initial work-up for acute liver failure is entirely unrevealing, and her liver function and hemodynamics improve without additional intervention over the initial 3 days of hospitalization. Unfortunately, her mental status does not improve. Despite weaning of all sedation, she shows limited signs of awareness. A lumbar puncture, CT of the head, and electroencephalogram (EEG) are performed and are unremarkable.
What should be done next? (Click on the correct answer to be directed to the second of six pages)
Cite as: Held N, Welsh C. October 2020 Critical Care Case of the Month: Unexplained Encephalopathy Following Elective Plastic Surgery. Southwest J Pulm Crit Care. 2020;21(4):73-9. doi: https://doi.org/10.13175/swjpcc041-20 PDF
October 2019 Critical Care Case of the Month: Running Naked in the Park
Spencer Jasper MD
Matthew Adams DO
Jonathan Boyd MD
Jeremiah Garrison MD
Janet Campion MD
The University of Arizona College of Medicine
Tucson, AZ USA
History of Present Illness
A 34-year-old man with a history of IV drug abuse was brought into emergency department by EMS and Tucson Police Department after complaints of naked man running and behaving erratically in a park. On arrival to emergency department patient was acting aggressively towards staff, spitting and attempting to bite. The ER staff attempted multiple times to sedate the patient with benzodiazepines, however, due to continued aggressive behavior, ongoing encephalopathy and the need for increased sedation, the patient was intubated for airway protection.
The patient was febrile (40.6° C), tachycardic (122) and hypertensive (143/86). On physical exam patient was not cooperative, was diaphoretic, cachectic, with reactive constrictive pupils, track marks in antecubital fossa bilaterally. No clonus or hypertonicity. During intubation, there was noted to be nuchal rigidity.
He was then admitted to the medical ICU. Drug intoxication from possible methamphetamines was the presumptive diagnosis of encephalopathy but given nuchal rigidity and fevers there was concern for other etiologies.
Physical Exam
- Vitals: T 40.6 °C, HR: 122, RR: 22, BP: 143/86, SpO2: 97% WT: 55 kg
- General: Intubated and sedated, cachectic
- Eye: Pupils constricted but reactive to light
- HEENT: Normocephalic, atraumatic
- Neck: Stiff, non-tender, no carotid bruits, no JVD, no lymphadenopathy
- Lungs: Clear to auscultation, non-labored respiration
- Heart: Normal rate, regular rhythm, no murmur, gallop or peripheral edema
- Abdomen: Soft, non-tender, non-distended, normal bowel sounds, no masses
- Skin: Skin is warm, dry and pink, multiple abrasions on the lower extremities bilaterally, track marks noted in the antecubital fossa bilaterally. Large abrasion with bruising around the right knee and erythema and welts on the right shin. Erythematous area on the dorsal surface of the right hand
- Neurologic: Nonfocal prior to intubation, no clonus or hypertonicity noted
Drug overdose/intoxication was presumptive diagnosis for his acute encephalopathy. Based on physical exam and vitals, what other etiologies should be considered? (click on the correct answer to be directed to the second of seven pages)
Cite as: Jasper S, Adams M, Boyd J, Garrison J, Campion J. October 2019 critical care case of the month: running naked in the park. Southwest J Pulm Crit Care. 2019;19(4):110-8. doi: https://doi.org/10.13175/swjpcc054-19 PDF
Corticosteroids and Influenza A associated Acute Respiratory Distress Syndrome
Philippe R. Bauer, MD, PhD
Vivek N. Iyer, MD, MPH
Pulmonary and Critical Care Medicine
Mayo Clinic
Rochester, MN USA
Abstract
The use of corticosteroids remains controversial in influenza infection, especially with lower respiratory tract infection. We present a case of moderate acute respiratory distress syndrome (ARDS) associated with influenza A that showed a dramatic improvement with combined corticosteroids and antiviral therapy. Host defense against virus infection consists of both innate and adaptive immune responses. An exuberant immune response to the primary pathogen leads to ‘collateral’ lung damage resulting in ARDS. The use of corticosteroids to modulate this excessive immune response, although intuitive, has been associated with increased mortality when administered early in the course of severe influenza A pneumonia. The administration of corticosteroids in this case was associated with a dramatic and unequivocal improvement. This unique case highlights the potential benefits of corticosteroids use in influenza A associated ARDS and may challenge clinicians to rethink current recommendations that specifically discourage corticosteroids use in patients with Influenza A associated ARDS.
Introduction
The impact of corticosteroids on clinical outcome in patients with influenza A associated respiratory failure is unclear (1). Retrospective studies suggest an adverse effect from early parenteral corticosteroids use in patients with pandemic influenza infection. On the other hand, in immunosuppressed patients, high dose corticosteroid given at the time of diagnosis of influenza was associated with a reduced risk for mechanical ventilation, without increased adverse effects other than delayed viral clearance. In general, the effect of corticosteroids on acute respiratory distress syndrome (ARDS) is controversial and its use is not routinely recommended. The adjunctive use of prednisone during the early phase of community-acquired pneumonia may actually reduce the development of ARDS (2). In severe influenza, early corticosteroids showed no evidence of benefit and suggested potential harm (3). We present a case of moderate ARDS associated with influenza A that showed a dramatic and unequivocal improvement after initiation of corticosteroids.
Abbreviations:
APACHE: Acute Physiology and Chronic Health Evaluation
ARDS: Acute Respiratory Distress Syndrome
ICU: Intensive Care Unit
PCR: Polymerase Chain Reaction
SOFA: Sequential Organ Failure Assessment
Case Report
A 62-year old male, nonsmoker, with a history of hypertension, dyslipidemia and depression, presented in March 2014 with chills, fever and nonproductive cough; he was initially treated for ‘bronchitis’ as an outpatient with levofloxacin. He had not received the influenza vaccine. Three days later, he developed acute hypoxemic respiratory failure with bilateral pulmonary infiltrates and was hospitalized elsewhere. Influenza testing was negative and he was started on piperacillin/tazobactam and azithromycin. He was transferred to our facility the next day because of worsening respiratory status. Initial heart rate was 80 bpm, blood pressure was 120/60 mm Hg, respirations was 22/min, and temperature was 37.7 ºC. The Acute Physiology and Chronic Health Evaluation (APACHE) IV score was 55 and the Sequential Organ Failure Assessment (SOFA) score was 8. His presentation was consistent with moderate ARDS with a PaO2/FiO2 ratio of 143, a chest radiograph showing bilateral pulmonary infiltrates (Figure 1) and no evidence of heart failure confirmed by bedside echocardiogram.

Figure 1. Bilateral pulmonary opacities consistent with moderate ARDS (PaO2/FiO2 ratio 143).
Nasal swab was again negative for influenza by polymerase chain reaction (PCR). Leukocyte count was 4.4 x 109/L with lymphopenia (0.22 x 109/L), hemoglobin was 11.7 g/dL, and platelet count was 216 x 109/L. Sodium was 134 mmol/L, creatinine was 1 mg/dL and AST was 142 U/L. He was initiated of high flow nasal oxygen, and vancomycin and oseltamivir were added. Due to the severity of his condition, he was also started on methylprednisolone (125 mg intravenously every 8 hours). After a brief trial of noninvasive ventilation, he was intubated, sedated, paralyzed and placed on a low tidal volume strategy with an initial PEEP of 15 cm H2O and a FiO2 of 0.7. A broncho-alveolar lavage, performed post intubation about 16 hours after admission to our facility, showed 35% alveolar macrophages, 8% lymphocytes and 57% neutrophils and was positive for influenza A by PCR; cultures were negative for other organisms. Other tests including HIV, RSV, Mycoplasma, Legionella and urine for Streptococcus antigen were all negative. The patient improved rapidly. He was extubated two days later, and continued on prednisone (40 mg daily) for five more days when he was dismissed home without any need for supplemental oxygen, although the chest radiograph continued to show infiltrates.
Discussion
This case illustrates a patient with delayed diagnosis and treatment of influenza A associated with moderate ARDS who made a rapid and complete recovery with antiviral, antibiotic and adjunctive high dose corticosteroid therapy.
The diagnosis of influenza A in this case meets all criteria established by Clinical Practice Guidelines of the Infectious Diseases Society of America (4). Rapid influenza testing lack sensitivity and false negative are not infrequent. ARDS is a well-defined complication of influenza infection. While the administration of corticosteroids appeared to temporally co-relate with clinical improvement, a causal link cannot be established definitively. The role of immunosuppression in influenza associated ARDS is very controversial with conflicting evidence from prospective (supportive) and retrospective (against) studies. For example, the combined use of sirolimus and prednisone was associated with significantly improved oxygenation as well as reduced organ dysfunction in mechanically ventilated patients with severe H1N1 respiratory failure (5). On the other hand, retrospective studies have shown increased mortality with the early use of high dose corticosteroids in severe influenza A pneumonia and respiratory failure. Furthermore, corticosteroids are now rarely used in ARDS and only sparingly given in case of refractory septic shock. The immune response to influenza infection depends on the virus, the host and the host response to infection. Host defense against virus infection consists of both innate and adaptive immune responses. An excessive immune response may result in ‘collateral damage’ and critical respiratory illness which may be ameliorated by the use of systemic corticosteroids. On the other hand, suppression of the host immune system may enhance viral replication and prolong critical illness. As a result of these conflicting data, major societies have been unable to firmly recommend for or against corticosteroids therapy in Influenza A associated respiratory failure.
In conclusion, we report on a case of Influenza A with ARDS and rapid improvement on corticosteroids. We have reviewed the current uncertainty surrounding the use of corticosteroids in this setting and leave open the possibility for careful consideration of this adjunctive therapy in other cases. Randomized trials are needed to further delineate the potential benefit of corticosteroids in severe influenza infection.
References
- Rodrigo C, Leonardi-Bee J, Nguyen-Van-Tam J, Lim WS. Corticosteroids as adjunctive therapy in the treatment of influenza. Cochrane Database Syst Rev. 2016 Mar 7;3:CD010406. [CrossRef] [PubMed]
- Blum CA, Nigro N, Briel M, et al. Adjunct prednisone therapy for patients with community-acquired pneumonia: a multicentre, double-blind, randomised, placebo-controlled trial. Lancet. 2015 Apr 18;385(9977):1511-8. [CrossRef] [PubMed]
- Brun-Buisson C, Richard JC, Mercat A, Thiébaut AC, Brochard L; REVA-SRLF A/H1N1v 2009 Registry Group. Early corticosteroids in severe influenza A/H1N1 pneumonia and acute respiratory distress syndrome. Am J Respir Crit Care Med. 2011 May 1;183(9):1200-6. [CrossRef] [PubMed]
- Harper SA, Bradley JS, Englund JA, et al. Seasonal influenza in adults and children--diagnosis, treatment, chemoprophylaxis, and institutional outbreak management: clinical practice guidelines of the Insert LinkInfectious Diseases Society of America. Clin Infect Dis. 2009 Apr 15;48(8):1003-32. [CrossRef] [PubMed]
- Wang CH, Chung FT, Lin SM, Huang SY, Chou CL, Lee KY, Lin TY, Kuo HP. Adjuvant treatment with a mammalian target of rapamycin inhibitor, sirolimus, and steroids improves outcomes in patients with severe H1N1 pneumonia and acute respiratory failure. Crit Care Med. 2014 Feb;42(2):313-21. [CrossRef] [PubMed]
Cite as: Bauer PR, Iyer VN. Corticosteroids and influenza A associated acute respiratory distress syndrome. Southwest J Pulm Crit Care. 2016;13(5):248-51. doi: https://doi.org/10.13175/swjpcc102-16 PDF
April 2016 Critical Care Case of the Month
Samir Sultan, DO
Banner University Medical Center Phoenix
Phoenix, AZ
Critical Care Case of the Month CME Information
Members of the Arizona, New Mexico, Colorado and California Thoracic Societies and the Mayo Clinic are able to receive 0.25 AMA PRA Category 1 Credits™ for each case they complete. Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Samir Sultan, DO. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives:
As a result of this activity I will be better able to:
- Correctly interpret and identify clinical practices supported by the highest quality available evidence.
- Will be better able to establsh the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Will improve the translation of the most current clinical information into the delivery of high quality care for patients.
- Will integrate new treatment options in discussing available treatment alternatives for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine
Current Approval Period: January 1, 2015-December 31, 2016
Financial Support Received: None
History of Present Illness
The patient is a 22-year-old African-American man who was initially seen following a rapid response team called to the neonatal intensive care unit for a seizure. He was visiting his newborn child. The nurses described the seizure as tonic-clonic which resolved spontaneously without treatment before the rapid response team arrived.
Past Medical History, Family History and Social History
The patient has a past medical history of a brain aneurysm treated by coil embolization 2 years earlier. He had no complications of the embolization including seizures. Family history is unremarkable. He smokes 1-2 cigars per day but does not drink alcohol.
Physical Examination
He was drowsy when initially seen but the drowsiness resolved in about 5 minutes. The physical examination was unremarkable and there were no focal neurologic signs.
What should be next? (Click on the correct answer to proceed to the second of seven panels)
- CT scan of the head
- Phenytoin administration
- Metabolic screening (BUN, glucose and electrolytes)
- 1 and 3
- All of the above
Cite as: Sultan S. April 2016 critical care case of the month. Southwest J Pulm Crit Care. 2016 Apr;12(4): . doi: http://dx.doi.org/10.13175/swjpcc033-16 PDF
March 2015 Critical Care Case of the Month: It’s Not Always Sepsis
Dionne Morgan, MD
Carolyn H. Welsh, MD
University of Colorado and the Eastern Colorado Veterans Affairs Medical Center
Department of Medicine
Division of Pulmonary Sciences and Critical Care Medicine
Denver, CO
History of Present Illness
A 57-year-old man with multiple co-morbidities including diabetes mellitus presented with wet gangrene of the right foot and hypotension. He had diabetic ketoacidosis and acute kidney injury. He was admitted to the medical intensive care unit, given intravenous fluids and treated with insulin therapy, piperacillin/tazobactam and vancomycin. Initial blood cultures grew Methicillin-resistant Staphylococcus aureus (MRSA). The podiatry service performed a right transmetatarsal amputation. Subsequently, he did well and was transferred to a medical floor for further care.
Three weeks later, following resolution of the initial sepsis, he developed persistently high fevers with hemodynamic instability despite continued antibiotic therapy. He was transferred back to the MICU for presumed sepsis.
Past Medical History, Social History and Family History
The past medical history was significant for diabetes, hypertension, COPD, coronary artery disease and hepatitis C. He did not smoke nor drink alcohol. Family history was non-contributory.
Physical Examination
On readmission to the medical intensive care unit, the patient was noted to have a generalized maculopapular rash on both upper and lower extremities, torso, palms and soles of his feet, associated with facial and periorbital edema (Figure 1). There was no mucosal membrane involvement or lymphadenopathy. He was also febrile to 104o F, hypotensive to 80/50 mm Hg and icteric.

Figure 1. Image of rash.
Laboratory Studies
Initial labs showed elevated leukocyte count, BUN and creatinine with anion-gap metabolic acidosis but a normal liver enzyme profile. Repeat labs on readmission to the medical ICU were significant for severe leukocytosis, with marked eosinophilia, atypical lymphocytes on blood smear, acute transaminitis and hyperbilirubinemia.
Admission labs: White blood cell count (WBC) 29.9 x 1000 cells/μL. Eosinophils 0.0% (Normal 0.0 - 0.7%), AST 28 U/L, ALT 15 U/L, ALP 162 U/L, total bilirubin 0.2 mg/dL.
Labs on ICU readmission: White blood cell count (WBC) 35.7 x 1000 cells/ μL. Eosinophils 2.3% (Normal 0.0 -0.7%), AST 486 U/L, ALT 288 U/L, ALP 749 U/L, total bilirubin 4.3 mg/dL.
Which are components of the SIRS criteria? (click on the correct answer to proceed to the second of 4 panels)
Reference as: Morgan D, Welsh CH. March 2015 critical care case of the month: it's not always sepsis. Southwest J Pulm Crit Care. 2015;10(3):105-11. doi: http://dx.doi.org/10.13175/swjpcc029-15 PDF
February 2015 Critical Care Case of the Month: A Bloody Mess
Mily Sheth, MD
Carmen Luraschi, MD
Matthew P. Schreiber, MD, MHS
University of Nevada School of Medicine: Las Vegas
Department of Internal Medicine
Division of Pulmonary/Critical Care
Las Vegas, NV
History of Presenting Illness:
A 23-year-old Ethiopian woman with a known history of systemic lupus erythematosus (SLE) but of unknown duration presented with the chief complains of cough and generalised weakness for 1 week. She had a recent history of travelling to Ethiopia 3 months ago for 3 weeks. She complained of subjective fevers and one episode of blood tinged sputum. She also complained of fatigue and an episode of syncope which prompted her hospitalization.
PMH, SH and FH:
The patient has a past medical history of SLE diagnosed in Ethiopia of which no records were available. She is a student and denied alcohol, smoking or drug abuse. She denied any family history of autoimmune disorders. She did not take any medications at home.
Physical Examination:
Initial admission vital signs were temperature of 100.5 F, heart rate of 130, respiratory rate of 30 and blood pressure of 92/48. Oxygen saturation was 96% on 2 L/min via nasal cannula.
She appeared to be in moderate distress but was speaking in full sentences. Skin examination revealed a malar rash on her face. Her upper and lower extremities had excoriated plaques. Her anterior chest had flat non blanchable, macular rash. CVS examination revealed tachycardia without any murmurs. Respiratory exam was positive for bilaterally diffuse bronchial breath sounds. The remainder of her exam was within normal limits.
Laboratory and Radiology:
CBC: WBC 6.7 million cells/mcL, hemoglobin 7.1 g/dL, hematocrit 20.9, platelet 160,000 cells/mcL
Renal panel: within normal limits.
Troponin 0.01, creatine kinase 457 U/L, lactic acid 1.1 mm/L, HIV non-reactive
Liver function tests: AST 288 U/L, ALT 93 U/L alkaline phosphatase 136 IU/L, total bilirubin 0.9 mg/dL
Radiography:
Her initial chest x-ray is shown in figure 1. It was interpreted as showing diffuse pulmonary infiltrates, right lung greater than left. No pleural effusions. No pneumothorax.

Figure 1. Initial chest x-ray.
In a patient with these characteristics, which other test(s) would you order? (Click on the correct answer to proceed to the second of five panels)
- Arterial blood gases and lactic acid
- Cardiac angiogram
- Computed tomography (CT) of the chest without contrast
- VATS lung biopsy
- All of the above
Reference as: Sheth M, Luraschi C, Schreiber MP. February 2015 critical care case of the month: a blood mess. Southwest J Pulm Crit Care. 2015;10(2):63-9. doi: http://dx.doi.org/10.13175/swjpcc148-14 PDF
December 2014 Critical Care Case of the Month: Weak for Weeks
Bhupinder Natt MD1
Shadi Koleilat MD2
Janet Campion MD1
1Division of Pulmonary, Allergy, Critical care and Sleep Medicine
2Department of Neurology
University of Arizona Medical Center
Tucson, AZ
History of Present Illness
A 65 year old woman presents with weakness involving both upper and lower extremities that is intermittent over the last 3 months, but in the last 2 weeks she has also noticed increasing neck weakness, droopy eyelids and increased drooling. Prior to this she was able to walk without difficulty and ride a recumbent bike for 20 minutes, but now is having difficulty walking on her own. She denies fevers, weight loss, shortness of breath, chest pain, palpitations, LE edema, joint pain, rash, any recent or current GI/GU symptoms and no new medications.
Past Medical History, Social History, and Family History
The patient has a past history of hypertension, hyperlipidemia, diabetes mellitus Type II, GERD, obstructive sleep apnea (compliant with BiPAP), atrial fibrillation and hypothyroidism. She has a 40 pack-year history of tobacco use. Family history is noncontributory.
Medications
- Dabigatran 75mg BID
- Esomeprazole 20 mg BID
- Furosemide 30 mg BID
- Insulin glargine 50 Units BID and Lispro per sliding scale
- Levothyroxine 88 mcg per day
- Losartan 50 mg QD,
- Pregabalin 75 mg BID
- Rosuvastatin 40 mg per day
Physical Examination
Vital signs: Afebrile. Pulse 86, respiratory rate 20, PaO2 92% on room air
General: Awake, fully oriented, dysarthric speech.
HEENT: Non-icteric, ears, nares, oropharynx unremarkable; there is no neck LAD, elevated JVP or thyromegaly.
Respiratory: Normal breath sounds, no wheeze or rhonchi.
CVS: Irregularly irregular rhythm, no murmurs. Peripheral vascular exam normal.
Abdomen: Obese, soft, non-tender with normal bowel sounds. No organomegaly appreciable.
Extremities: Trace pedal edema, normal muscle bulk and tone.
CN: Ptosis bilaterally, no nystagmus, reactive pupils, extra-ocular muscles intact, sensation intact, weak cheek puff, symmetric palate excursion, normal tongue protrusion.
Motor: Neck flexion and extension 4-/5, bilateral pronator drift, no focal lower extremity weakness, no muscle atrophy, no tremors or fasciculations.
Sensation: Intact to light touch hands and feet.
Reflexes: 2+ and symmetric throughout.
Gait: Wide-based and slow, can only walk short distances before experiencing bilateral leg weakness.
Laboratory: Normal electrolytes, complete blood count, and liver function tests. Creatinine mildly elevated at 2.1 mg/dL.
EKG
Atrial Fibrillation.
What is the most likely diagnosis? (Click on the correct answer to proceed to the next panel)
- Guillain-Barré syndrome (GBS)
- Hypothyroidism
- Lambert-Eaton myasthenic syndrome (LEMS)
- Motor neuron disease (ALS)
- Myasthenia gravis crisis
Reference as: Natt B, Koleilat S, Campion J. December 2014 critical care case of the month: weak for weeks. Southwest J Pulm Crit Care. 2014;9(6):302-8. doi: http://dx.doi.org/10.13175/swjpcc141-14 PDF
January 2013 Critical Care Case of the Month: Different Name, Same Disease...or Is It?
Nathaniel Reyes MD (NReyes@deptofmed.arizona.edu)
Jarrod Mosier MD (JMosier@aemrc.arizona.edu)
University of Arizona- AHSC/Pulmonary
1501 N Campbell Ave.
Tucson, AZ 85724-5030
History of Present Illness
A 50-year-old female who presented with 2-weeks of worsening cough and shortness of breath. She presented to another hospital 2-weeks prior to presentation complaining of cough productive of yellow sputum and was diagnosed with bronchitis and discharged home with a normal chest x-ray. Her symptoms persisted and one day prior to admission she experienced one episode of hemoptysis which prompted her presentation to our emergency department. She denied fever, chills, night sweats, and complained only of dyspnea on exertion.
PMH/SH
Granulomatous polyangitis (GPA) was diagnosed by renal biopsy in 2004. She subsequent developed end-stage renal disease and has been receiving peritoneal dialysis. She has never required immunosuppresive therapy. There is no history of tobacco use. She has lived in Arizona for many years. She is retired but previously worked as an information technology manager.
Physical Exam
Vital signs were normal except for an O2 saturation of 91% on room air. Physical exam was significant only for pale sclerae and bilateral dry crackles.
Laboratory Data
Hemoglobin: 5.4 g/dL; Hematocrit: 17%. BUN: 43 mg/dL; creatinine: 10.7 mg/dL.
ABG: PaO2 75; PaCO2 39; pH 7.43 on 2L O2.
P-ANCA: Positive
Myeloperoxidase antibody titer: 83 U/mL
C-ANCA/proteinase 3 antibody titer/Anti-GBM antibodies: negative.
Imaging
Chest X-ray showed diffuse areas of consolidation (Figure 1).

Figure 1. PA Chest X-ray
Which of the following is not appropriate in her management?
The authors report no conflict of interest.
Reference as: Reyes N, Mosier J. Critical care case of the month: different name, same disease...or is it? Southwest J Pulm Crit Care 2013;6(1):5-11. PDF