
Critical Care
The Southwest Journal of Pulmonary and Critical Care publishes articles directed to those who treat patients in the ICU, CCU and SICU including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.

The Effect of Low Dose Dexamethasone on the Reduction of Hypoxaemia and Fat Embolism Syndrome After Long Bone Fractures
Dr. Akash K
Dr. Madhuchandra R
Department Of Orthopaedics, Karnataka Institute Of Medical Sciences, Hubli, India
Abstract
Background: A dangerous and sometimes fatal consequence of post-traumatic long bone fractures is fat embolism syndrome (FES). The reported incidence of FES ranges from 2% to 22%. FES can also lead to critical illness with fatality rates between 10 to 36%. This study's objective was to determine whether prophylaxis of the fat emboli syndrome could be achieved with lower doses of dexamethasone than had previously been recommended. Thus, prevention of respiratory insufficiency and disruption of homeostasis are essential.
Methods: A total of 583 adult cases of long bone shaft fracture patients between January 2020 to December 2021 were randomly divided into a trial group (n= 252) and a control group (n=331) by simple randomization. The trial group received dexamethasone 8mg/day for 3 days and the control group was given placebo. FES was diagnosed using Gurd’s diagnostic criteria and the FES morbidity and death rates in each group were examined.
Results: Five patients (0.151%) in the control group and 1 patient (0.39%) in the trial group developed FES but the difference was not significant (p>0.05). SpO2 values were significantly elevated in the dexamethasone-treated group compared to the control group 24 hours after admission (p<0.05) and the elevation persisted on the third post admission day (p<0.05).
Conclusion: Dexamethasone in low doses reduces post-traumatic hypoxia in patients with long bone fracture. However, our study was underpowered to show a reduction in FES.
Introduction
Fat emboli occur in all long bone fractures with the most severe resulting in fat embolism syndrome (FES). The reported incidence of FES ranges from 2% to 22% with fatality rates of 10-36% (1-3) with FES resulting in the adult respiratory distress syndrome a 50–90% mortality rate (1-3). Unfortunately, this is particularly common in young people in their second and third decades of life who sustain polytrauma and/or femur fractures in high-velocity traffic accidents (2,3). The majority of trauma patients may experience a subclinical form of FES, which manifests as hypoxaemia alone (3-6).
FES resulting in systemic symptoms is a rare clinical outcome. Following a traumatic incident, fat droplets are released into the bloodstream resulting in fat embolization. This results in immediate tissue damage as well as a systemic inflammatory response that produces symptoms in the lungs, skin, nervous system, and retina (7,8). Most instances of FES occur after trauma but rare cases of FES have been reported to occur after bone marrow transplantation, osteomyelitis, pancreatitis, alcoholic fatty liver, and even liposuction (9,10). Although the classic triad of pulmonary distress, mental status changes, and petechial rash is usually not seen, hypoxia 24 to 48 hours after pelvic or long-bone fractures is common (11-13).
FES has no pathognomonic characteristics and laboratory and radiographic findings are nonspecific (14,15). Early detection of FES may allow supportive pulmonary treatment and other life-saving interventions to stop the pathophysiologic cascade and stop clinical deterioration. The majority of curative methods created expressly for FES have failed (16,17). There have been several attempts to avoid FES since it is such a serious issue in trauma patients (4). With varying degrees of success, heparin, dextran, albumin, hypertonic glucose, aspirin, and early fracture stabilization, have all been attempted (4). Steroids have also been studied as a preventative as well as a therapeutic agent in fat embolism in various studies.
When fat droplets act as emboli and are trapped in the pulmonary microvasculature and other microvascular beds, such as the brain, they may cause clinical symptoms to appear 24-72 hours after trauma (and particularly after fractures). Embolization starts out very slowly and reaches its peak in 48 hours or more. A long-acting corticosteroid having a half-life of 36 to 72 hours is dexamethasone. This study's objective was to determine whether prophylaxis of the fat emboli syndrome could be achieved with lower doses of dexamethasone than had previously been recommended (17).
Patients and Methods
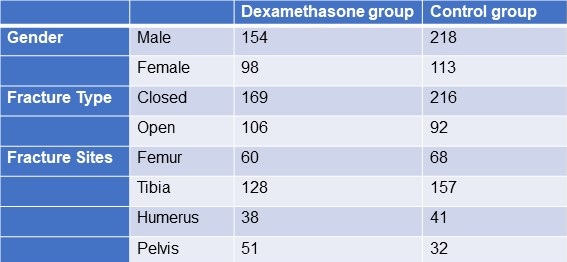
From January 2020 to December 2021, 583 adult patients between the ages of 18 and 60 with long bone fractures without a history of chronic heart, lung, liver, or renal failure were recruited from patients at KIMS Hospital Hubli. There were 211 cases observed in women and 372 cases in men. The injuries resulted from motor accidents (426), falls (127), and crush injuries (30). Fracture sites included 128 femur fractures, 285 tibia and fibula fractures, 79 humerus fractures, and 91 pelvic injuries. The patients were randomized into two groups, one receiving dexamethasone and the other receiving a placebo (Table 1).
Table 1. Demographic data

Click here to display Table 1 in a separate, enlarged window.
{kind=link}
The following patient information was recorded: gender, age, weight, time from injury to admission, primary fracture location, type of fracture, FES morbidity, and number of fatalities. All patients received traditional medical care, early hypovolemic shock correction, fracture stabilization, and symptomatic therapy (2). The trial group received dexamethasone 8mg/day for 3 days and the control group was given placebo. All patients were monitored (heart rate, BP, SpO2 ,respiratory rate, urine output, and arterial blood gases) every 6 hours for 3 days. We considered hypoxaemia with any pO2 <70mm Hg and classified all patients in 3 categories; severe (pO2<60mm Hg), mild hypoxaemia (pO2 >60- <70 mm Hg) and normal (pO2>70mm Hg). All patients signed an informed consent form. The study was approved by the Ethics Committee of our institute hospital.
Treatment and diagnosis for FES
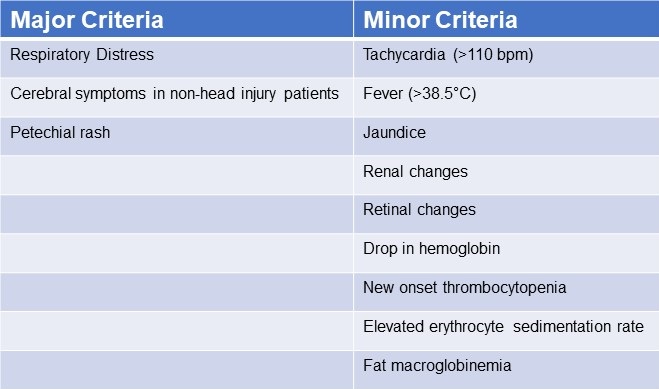
Patients were identified using “Gurd’s Diagnostic criteria score”(Table 2), and those whose score was 2 major or 1 major and 4 minor were diagnosis as FES.
Table 2. Gurd’s Diagnostic Criteria Score*

*Two major criteria or 1 major criterion and 4 minor criteria suggest a diagnosis of FES. Click here to view Table 2 in a separate and enlarged window.
{kind=link}
Data analysis
Utilizing statistical tools, the analysis was conducted (SPSS 20.0). P< 0.05 was regarded as statistically significant when comparing the patients' age, main fracture location, fracture type, and incidence of FES using the chi-squared test and single-factor analysis of variance, respectively.
Results
FES occurred in the dexamethasone group and control group, with 1 and 5 cases, respectively (Table 3). Statistical analysis revealed that there was no statistically significant difference between the groups for sex, age, weight, injury to admission time, main fracture site, fracture type, or medication time.
Table 3. Incidence of FES
 Click here to view Table 3 in a separate, enlarged window.
Click here to view Table 3 in a separate, enlarged window.
{kind=link}
Twenty-four hours after admission, steroid treated patients displayed a statistically significant higher PaO2 value compared to the control group (p<0.05) and this difference persisted through the 3rd post admission day (p<0.05, table 4).
Table 4. Partial pressures of oxygen (in mm Hg) in patients treated with IV dexamethasone and controls.

Click here to view Table 4 in a separate and enlarged window.
{kind=link}
Discussion
Much higher dosages of dexamethasone have been used to treat some pathological conditions in order to reduce inflammation, inhibit the immune system, impact the hemopoietic system, and alter metabolism (18-28). The mechanical-chemical hypothesis of fat embolism hypothesizes that neutral triglycerides are hydrolyzed into glycerol and free fatty acids by lipoprotein lipase from the lungs. The free fatty acids lead to inflammation and endothelial damage. Corticosteroids likely act on FES by reducing this inflammation. Due to a lack of clear diagnostic markers, treating FES may prove challenging. There have been few publications on the use of adrenal steroids to prevent high-risk FES patients, although the results have been ambiguous at low doses (31). Observational clinical research revealed that short-range and high doses may be helpful in reducing plasma free fatty acid concentrations, maintaining PaO2 levels, and reducing the occurrence of long bone fractures in individuals with FES. Dexamethasone may be a more effective drug treatment for FES (32). The dose of dexamethasone used in our study was relatively small and short, and complications related to hormones such as stress ulcer, aseptic necrosis of the femoral head, and bleeding tendency did not occur. It should be noted that drug prevention must be based on early, accurate fracture fixation, early corrective hypovolemic shock, and other standard procedures (33). This is true even if drug usage in this population clearly has a preventative impact. Ashbaugh and Petty (34) suggested corticosteroid therapy for treating FES in 1966 and gave laboratory data proving its therapeutic impact in the experimental animal given an intravenously administered FFA injection. Rokkanen et al. (35) found that 5 mg/kg of dexamethasone administered at 1 and 48 h after burn injury failed to enhance nuclear translocation of the GR, and to suppress the overproduction of proinflammatory cytokines such as TNF-α and IL-1β, neither did it increase the release of anti-inflammatory cytokine IL-10. In experiments with animals, Kreis et al. (36) showed that corticosteroids increased oxygenation and lowered the pathological alterations seen in lung biopsies. Alho et al. (37) conducted research on the use of intravenous methyl prednisolone sodium succinate in the prevention of fat embolism syndrome. A total of 60 individuals with at least two fractures were included in his study (pelvic, femoral or tibial fractures).methyl prednisolone reduces signs of hypoxaemia, bilateral "snow storm" infiltrations of the lungs, petechial rash, mental disturbances, pyrexia, anemia and thrombocytopenia. Varying degrees of the syndrome were observed in two patients given methylprednisolone and in 15 patients in the control group. Babalis et al. (39) results support the prophylactic administration of methylprednisolone in small dosage to prevent post traumatic hypoxaemia and probably FES in patients with isolated lower limb long bone fractures, especially when early fracture stabilization is not possible. Therefore, every study has demonstrated the effectiveness of steroids as a preventative treatment for the fat embolism syndrome.
Although our results showed a trend towards reduction in FES after long bone fractures, the results were not statistically significant. This is likely because our study turned out to be underpowered. We had anticipated an incidence of FES between 2-20% reported in the literature rather than the 1.1% found in our study.
Conclusion
The study's objective was to determine whether prophylaxis of the fat emboli syndrome could be achieved with lower doses of dexamethasone than had previously been recommended. Among the several prophylactic drugs that have been researched so far for the fat embolism syndrome, dexamethasone have shown to be relatively beneficial. The frequency of hypoxaemia and fat emboli syndrome decreased with intravenous dexamethasone at 8 mg per day for three days. Dexamethasone is a long-acting symptoms that emerge 24-72 hours after trauma (and particularly after fractures). Fat embolization begins slowly and reaches its maximum around 48 hours.
The limitation of our study is that it lacked sufficient power to demonstrate a reduction in FES. Furthermore, no method has been developed to pinpoint precisely who could benefit from steroid prophylaxis. We based our study assuming an incidence of FES of about 5%. However, we found an incidence of only about 1.5%. The lower incidence is probably due to our use of Gurd’s criteria which is more restrictive than the criteria used in other studies. Based on our observed incidence of FES of 1.5% with a reduction to 0.4% we estimate that over 2500 patients would be needed to show a statistically significant reduction in FES.
Our study shows that hypoxaemia is reduced by a relatively low dose of dexamethasone administered for a relatively short length of time. It may prevent FES but our study was underpowered to show a difference.
Declaration
Human subjects: Consent was obtained or waived by all participants in this study. Karnataka Institute Of Medical Sciences ethics committee. issued approval 327/2020-21. The study was approved by the institutional ethics committee. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissues. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all
authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work
References
- Sproule BJ. Brady JL. Gilbert J. Studies on the Syndrome of Fat Embolization. Can Med Assoc J. 1964 May 30;90(22):1243-7. [PubMed]
- Wertzberger JL, Peltier LF. Fat embolism: the importance of arterial hypoxia. Surgery. 1968 Apr;63(4):626-9. [PubMed]
- Stürm JA, Lewis FR Jr, Trentz O, Oestern HJ, Hempelman G, Tscherne H. Cardiopulmonary parameters and prognosis after severe multiple trauma. J Trauma. 1979 May;19(5):305-18. [CrossRef] [PubMed]
- Hutchins PM, Macnicol MF. Pulmonary insufficiency after long bone fractures. Absence of circulating fat or significant immunodepression. J Bone Joint Surg Br. 1985 Nov;67(5):835-9. [CrossRef] [PubMed]
- Levy D. The fat embolism syndrome. A review. Clin Orthop Relat Res. 1990 Dec;(261):281-6. [PubMed]
- Gossling HR, Pellegrini VD Jr. Fat embolism syndrome: a review of the pathophysiology and physiological basis of treatment. Clin Orthop Relat Res. 1982 May;(165):68-82. [PubMed]
- Kwiatt ME, Seamon MJ. Fat embolism syndrome. Int J Crit Illn Inj Sci. 2013 Jan;3(1):64-8. [CrossRef] [PubMed]
- Parisi DM, Koval K, Egol K. Fat embolism syndrome. Am J Orthop (Belle Mead NJ). 2002 Sep;31(9):507-12. [PubMed]
- Scuderi CS. The present status of fat embolism. Bibliographic review. Int Surg Digest 1934; 18: 195-215.
- Gurd AR. Fat embolism: an aid to diagnosis. J Bone Joint Surg Br. 1970 Nov;52(4):732-7. [PubMed]
- Nixon JR, Brock-Utne JG. Free fatty acid and arterial oxygen changes following major injury: a correlation between hypoxaemia and increased free fatty acid levels. J Trauma. 1978 Jan;18(1):23-6. [CrossRef] [PubMed]
- Parker FB Jr, Wax SD, Kusajima K, Webb WR. Hemodynamic and pathological findings in experimental fat embolism. Arch Surg. 1974 Jan;108(1):70-4. [CrossRef] [PubMed]
- Nijsten MW, Hamer JP, ten Duis HJ, Posma JL. Fat embolism and patent foramen ovale. Lancet. 1989 Jun 3;1(8649):1271. [CrossRef] [PubMed]
- Vedrinne JM, Guillaume C, Gagnieu MC, Gratadour P, Fleuret C, Motin J. Bronchoalveolar lavage in trauma patients for diagnosis of fat embolism syndrome. Chest. 1992 Nov;102(5):1323-7. [CrossRef] [PubMed]
- White T, Petrisor BA, Bhandari M. Prevention of fat embolism syndrome. Injury. 2006 Oct;37 Suppl 4:S59-67. [CrossRef] [PubMed]
- Laterre PF, Wittebole X, Dhainaut JF. Anticoagulant therapy in acute lung injury. Crit Care Med. 2003 Apr;31(4 Suppl):S329-36. [CrossRef] [PubMed]
- Bederman SS, Bhandari M, McKee MD, Schemitsch EH. Do corticosteroids reduce the risk of fat embolism syndrome in patients with long-bone fractures? A meta-analysis. Can J Surg. 2009 Oct;52(5):386-93. [PubMed]
- McEvoy GK, Snow EK, Kester L, eds. AHFS 2002 Drug Information. Bethesda, MD: American Society of Health‐System Pharmacists; 2002.
- Chamberlain D. Emergency medical treatment of anaphylactic reactions. Project Team of the Resuscitation Council (UK). J Accid Emerg Med. 1999 Jul;16(4):243-7. [CrossRef] [PubMed]
- Niermeyer S, Kattwinkel J, Van Reempts P, et al. International Guidelines for Neonatal Resuscitation: An excerpt from the Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care: International Consensus on Science. Contributors and Reviewers for the Neonatal Resuscitation Guidelines. Pediatrics. 2000 Sep;106(3):E29. [CrossRef] [PubMed]
- Brun-Buisson C, Brochard L. Corticosteroid therapy in acute respiratory distress syndrome: better late than never? JAMA. 1998 Jul 8;280(2):182-3. [CrossRef] [PubMed]
- Hudson LD. New therapies for ARDS. Chest. 1995 Aug;108(2 Suppl):79S-91S. [CrossRef] [PubMed]
- Meduri GU, Headley AS, Golden E, Carson SJ, Umberger RA, Kelso T, Tolley EA. Effect of prolonged methylprednisolone therapy in unresolving acute respiratory distress syndrome: a randomized controlled trial. JAMA. 1998 Jul 8;280(2):159-65. [CrossRef] [PubMed]
- Johnson MJ, Lucas GL. Fat embolism syndrome. Orthopedics. 1996 Jan;19(1):41-8; discussion 48-9. [CrossRef] [PubMed]
- Kallenbach J, Lewis M, Zaltzman M, Feldman C, Orford A, Zwi S. 'Low-dose' corticosteroid prophylaxis against fat embolism. J Trauma. 1987 Oct;27(10):1173-6. [PubMed]
- Niewoehner DE, Erbland ML, Deupree RH, Collins D, Gross NJ, Light RW, Anderson P, Morgan NA. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med. 1999 Jun 24;340(25):1941-7. [CrossRef] [PubMed]
- Richards RR. Fat embolism syndrome. Can J Surg. 1997 Oct;40(5):334-9. [PubMed]
- Kubota T, Ebina T, Tonosaki M, Ishihara H, Matsuki A. Rapid improvement of respiratory symptoms associated with fat embolism by high-dose methylpredonisolone: a case report. J Anesth. 2003;17(3):186-9. [CrossRef] [PubMed]
- Han YY, Sun WZ. An evidence-based review on the use of corticosteroids in peri-operative and critical care. Acta Anaesthesiol Sin. 2002 Jun;40(2):71-9. [PubMed]
- Habashi NM, Andrews PL, Scalea TM. Therapeutic aspects of fat embolism syndrome. Injury. 2006 Oct;37 Suppl 4:S68-73. [CrossRef] [PubMed]
- Babalis GA, Yiannakopoulos CK, Karliaftis K, Antonogiannakis E. Prevention of posttraumatic hypoxaemia in isolated lower limb long bone fractures with a minimal prophylactic dose of corticosteroids. Injury. 2004 Mar;35(3):309-17. [CrossRef] [PubMed]
- Yamamoto T, Irisa T, Sugioka Y, Sueishi K. Effects of pulse methylprednisolone on bone and marrow tissues: corticosteroid-induced osteonecrosis in rabbits. Arthritis Rheum. 1997 Nov;40(11):2055-64. [CrossRef] [PubMed]
- Talbot M, Schemitsch EH. Fat embolism syndrome: history, definition, epidemiology. Injury. 2006 Oct;37 Suppl 4:S3-7. [CrossRef] [PubMed]
- Ashbaugh DG, Petty TL. The use of corticosteroids in the treatment of respiratory failure associated with massive fat embolism. Surg Gynecol Obstet. 1966 Sep;123(3):493-500. [PubMed]
- Rokkanen P, Alho A, Avikainen V, Karaharju E, Kataja J, Lahdensuu M, Lepistö P, Tervo T. The efficacy of corticosteroids in severe trauma. Surg Gynecol Obstet. 1974 Jan;138(1):69-73. [PubMed]
- Kreis WR, Lindenauer SM, Dent TL. Corticosteroids in experimental fat embolization. J Surg Res. 1973 Mar;14(3):238-46. [CrossRef] [PubMed]
- Alho A, Saikku K, Eerola P, Koskinen M, Hämäläinen M. Corticosteroids in patients with a high risk of fat embolism syndrome. Surg Gynecol Obstet. 1978 Sep;147(3):358-62. [PubMed]
- Stoltenberg JJ, Gustilo RB. The use of methylprednisolone and hypertonic glucose in the prophylaxis of fat embolism syndrome. Clin Orthop Relat Res. 1979 Sep;(143):211-21. [PubMed]
- Babalis GA, Yiannakopoulos CK, Karliaftis K, Antonogiannakis E. Prevention of posttraumatic hypoxaemia in isolated lower limb long bone fractures with a minimal prophylactic dose of corticosteroids. Injury. 2004 Mar;35(3):309-17. [CrossRef] [PubMed]
A Case and Brief Review of Bilious Ascites and Abdominal Compartment Syndrome from Pancreatitis-Induced Post-Roux-En-Y Gastric Remnant Leak
Marissa A. Martin, MD1
Michael H. Lee, MD2
Anna Neumeier, MD3
Tristan J. Huie, MD3
1 University of Colorado Department of Internal Medicine
2 University of California, San Francisco Division of Pulmonary and Critical Care Medicine
3 University of Colorado Division of Pulmonary Sciences and Critical Care Medicine
Abstract
This is a case of a 55-year-old man with Roux-en-Y gastric bypass surgery 15 years prior who presented with acute pancreatitis and developed distributive shock, bacteremia, acute respiratory distress syndrome, anuric acute renal failure, and a distended abdomen with increasing ascitic fluid on imaging. An elevated bladder pressure, lactic acidosis, and anuria raised concern for abdominal compartment syndrome. Paracentesis was done and four liters of bilious ascitic fluid were drained. Intra-abdominal pressure was measured and improved from 27 cmH2O to 13 cmH2O with paracentesis. Mean arterial pressure and urine output also improved. The patient developed recurrent loculated intra-abdominal fluid collections, though ultrasound, CT scans with and without contrast, MRCP, ERCP, upper GI fluoroscopy, and small bowel enteroscopy failed to reveal a source of the bilious output. Ultimately, a gastrostomy tube was placed and delivery of contrast material through the tube revealed active extravasation from the remnant stomach. This case underscores the importance of considering post-surgical leak regardless of how remotely a Roux-en-Y surgery took place, confirms the importance of pursuing early gastrostomy tube placement and contrast administration when post-Roux-en-Y gastric remnant leaks are suspected, and demonstrates the role of paracentesis in critically ill patients with abdominal compartment syndrome.
Background
Post-surgical leaks complicate up to 7% of Roux-en-Y gastric bypass procedures and they result in greater than 50% morbidity and mortality (1,2). Most leaks (between 69% and 77%) occur at the gastrojejunal anastomosis, and on average, they become symptomatic three days after surgery (3,4). Rare leaks from the gastric remnant, which is the larger portion of the stomach that during a Roux-en-Y surgery is bypassed with the gastrojejunal anastomosis, have been reported and have been said to have delayed presentations, though this has typically only been weeks after surgery, not years (1,5). This is a case of post-Roux-en-Y gastric remnant leak that occurred 15 years after the original surgery, underscoring the importance of considering post-surgical leak as a diagnostic possibility regardless of how remotely a Roux-en-Y surgery took place. This case discusses a possible provoking factor, illustrates the clinical presentation, and suggests a diagnostic and treatment approach for these leaks. As morbid obesity becomes more prevalent in today’s society and Roux-en-Y gastric bypass procedures become even more mainstream, knowledge of delayed complications, such as the one discussed in this case, is crucial.
Case Report
A 55-year-old man with a past medical history of atrial fibrillation, previous alcohol-induced acute pancreatitis, and Roux-en-Y gastric bypass surgery 15 years prior presented with three days of abdominal pain and pre-syncope. He was drinking four to five alcoholic drinks daily. On presentation to the emergency department, the patient was in atrial fibrillation with a heart rate greater than 160 beats/min and was hypotensive to 77/53 mmHg. He was afebrile and mildly leukopenic with a white blood cell count of 4.4 k/mL. He had a lactate level of 12.5 mmol/L and a lipase of 1756 U/L with clinical and radiographic evidence of acute pancreatitis (Figure 1).

Figure 1. CT scan showing an enlarged pancreatic head and proximal body (arrow) with peripancreatic fat stranding (arrowhead), consistent with acute pancreatitis.
He was admitted to the medical intensive care unit, where over the next two days his distributive shock was complicated by Enterobacter cloacae bacteremia, acute respiratory distress syndrome, and acute anuric renal failure. For the management of his multi-organ failure, the patient was placed on mechanical ventilation, paralytic therapy, and infusions of norepinephrine, vasopressin, and phenylephrine. He was also started on continuous renal replacement therapy.
On hospital day three, the patient developed increasing abdominal distention with CT showing an interval increase in the size of ascites. An elevated bladder pressure of 21 mmHg, measured following the administration of rocuronium, along with a lactate of 12.3 mmol/L and anuria raised the concern for abdominal compartment syndrome. Paracentesis was done and four liters of bilious ascitic fluid were drained (Figure 2).

Figure 2. Paracentesis drained four liters of bilious fluid. Using a manometer, intra-abdominal pressure was measured first prior to fluid removal and subsequently after each liter was drained. The intra-abdominal pressure was 27 cmH2O initially and decreased to 13 cmH2O.
Using the manometer from a lumbar puncture kit, intra-abdominal pressure was measured first prior to fluid removal and subsequently after each liter was drained. With fluid removal, the initial intra-abdominal pressure of 27 cmH2O improved to 13 cmH2O (Figure 2), and the mean arterial pressure increased by 16 mmHg (from 70 mmHg to 86 mmHg). The norepinephrine, which had been infusing at 0.1 mcg/kg/min, was discontinued over the subsequent hour and a half, and the patient maintained a mean arterial pressure of 85 mmHg. Over the subsequent 12 hours, the patient’s urine output increased, and continuous renal replacement therapy was discontinued. Analysis of the ascitic fluid showed significantly elevated total bilirubin (17 mg/dL), lactate dehydrogenase (3545 U/L), and amylase (1481 U/L). Serum ascites albumin gradient was 1.1.
Over the next two weeks, the patient developed recurrent loculated intra-abdominal fluid collections (Figure 3) and leukocytosis (as high as 31.9 k/mL) refractory to two additional paracenteses with large volume ascitic fluid removal and broad-spectrum antibiotic treatment.

Figure 3. CT scan showing recurrent loculated intra-abdominal fluid collections (arrow) despite broad spectrum antibiotics and repeated paracenteses.
For definitive management of the recurrent ascites, two intra-abdominal drains were placed with fluid cultures growing Candida albicans. Intravenous micafungin was started, which was later narrowed to oral fluconazole. Continued high bilious output from the drains (as high as 3 L daily) raised the suspicion for biliary perforation or a post-Roux-en-Y leak. Multiple imaging studies including ultrasound, CT scans with and without contrast, and magnetic resonance cholangiopancreatography (MRCP), however, did not reveal a source of the bilious output. Although a hepatobiliary iminodiacetic acid (HIDA) scan showed a large leakage at the gastrojejunal anastomotic site, subsequent endoscopic retrograde cholangiopancreatography (ERCP), upper GI fluoroscopy, and small bowel enteroscopy did not demonstrate an overt contrast leak. Ultimately, a gastrostomy tube was placed by interventional radiology and delivery of contrast material through the tube revealed an active extravasation from the remnant stomach (Figure 4).

Figure 4. CT scan showing extravasated contrast material (arrows) from the patient’s remnant stomach.
The patient was eventually discharged home on hospital day 28 with one remaining intra-abdominal drain in addition to the gastric tube to allow for gastric decompression and spontaneous healing of the post-Roux-en-Y leak.
Discussion
As discussed in the introduction, post-surgical leaks are a known complication of Roux-en-Y gastric bypass procedures and they have great morbidity and mortality. They most commonly occur at the gastrojejunal anastomosis and are typically detected within days of the original surgery. In our patient, it is likely that his alcohol-induced acute pancreatitis triggered the release of activated proteolytic pancreatic enzymes, which resulted in the gastric remnant leak and infected bilious ascites, a pathophysiologic mechanism previously suggested by one case series (6). Our patient’s delayed presentation 15 years after his Roux-en-Y gastric bypass surgery underscores the importance of considering post-surgical leak as a diagnostic possibility regardless of how remotely the surgery took place.
Diagnosing post-Roux-en-Y gastric remnant leaks can remain challenging even when they are suspected. Our patient’s gastric remnant leak was identified only after contrast delivery through the gastrostomy tube; previous diagnostic studies, including ultrasound, CT scans with and without contrast, MRCP, ERCP, upper GI fluoroscopy, and small bowel enteroscopy were all non-diagnostic. Similar diagnostic difficulty was described in another case of gastric remnant leak also complicated by the formation of amylase-containing dark ascitic fluid, in which the correct diagnosis was made only with CT-guided percutaneous gastrostomy followed by administration of contrast material (5). We hypothesize that this diagnostic difficulty is due to the inability of enteral contrast to reach the decompressed gastric remnant in adequate volume to detect a perforation, since it would be required to move against the typical flow of gastric secretions after a Roux-en-Y procedure. Our case confirms the importance of pursuing early gastrostomy tube placement and contrast administration when post-Roux-en-Y gastric remnant leak is suspected in order to allow for definitive diagnosis and appropriate treatment.
This case also highlights the diagnostic utility of paracentesis in abdominal hypertension or abdominal compartment syndrome, defined as an intra-abdominal pressure ≥ 12 mmHg or an intra-abdominal pressure > 20 mmHg with new organ dysfunction, respectively (7). Although our patient’s distended abdomen, elevated bladder pressure, and anuria collectively raised the concern for abdominal compartment syndrome, his abdomen remained soft. We therefore pursued paracentesis rather than exploratory laparotomy to both achieve an accurate assessment of the intra-abdominal pressure and drain the ascitic fluid. Our patient’s initial intra-abdominal pressure was 27 cmH2O (equivalent to 20 mmHg, similar to the patient’s paralyzed bladder pressure of 21 mmHg), which decreased to 13 cmH2O (or 9.6 mmHg) after four liters of fluid were removed. There was also clear evidence of improvement in end-organ perfusion and function after the paracentesis. We demonstrated a diagnostic as well as therapeutic role of paracentesis in critically ill patients with abdominal compartment syndrome. We showed that paracentesis is a viable alternative to surgical laparotomy, particularly when objective data such as bladder pressure does not correspond with physical examination findings.
References
- Strobos E, Bonanni F. Asymptomatic gastric remnant leak after laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2009 Sep-Oct;5(5):630-2. [CrossRef] [PubMed]
- Madan AK, Lanier B, Tichansky DS. Laparoscopic repair of gastrointestinal leaks after laparoscopic gastric bypass. Am Surg. 2006 Jul;72(7):586-90; discussion 590-1. [PubMed]
- Levine MS, Carucci LR. Imaging of bariatric surgery: normal anatomy and postoperative complications. Radiology. 2014 Feb;270(2):327-41. [CrossRef] [PubMed]
- Lim R, Beekley A, Johnson DC, Davis KA. Early and late complications of bariatric operation. Trauma Surg Acute Care Open. 2018 Oct 9;3(1):e000219. [CrossRef] [PubMed]
- Karmali S, Azer N, Sherman V, Birch DW. Computed tomography-guided percutaneous gastrostomy for management of gastric remnant leak after Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2011 Mar-Apr;7(2):227-31. [CrossRef] [PubMed]
- Schein M, Saadia R, Decker GA. Postoperative pancreatitis--a cause of anastomotic leaks? A report of 4 cases. S Afr Med J. 1988 May 7;73(9):550-1. [PubMed]
- Kirkpatrick AW, Roberts DJ, De Waele J, et al. Intra-abdominal hypertension and the abdominal compartment syndrome: updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med. 2013 Jul;39(7):1190-206. [CrossRef] [PubMed]
Cite as: Martin MA, Lee MH, Neumeier A, Huie TJ. A case and brief review of bilious ascites and abdominal compartment syndrome from pancreatitis-induced post-Roux-en-Y gastric remnant leak. Southwest J Pulm Crit Care. 2021;23(1):18-22. doi: https://doi.org/10.13175/swpcc018-21 PDF
January 2020 Critical Care Case of the Month: A Code Post Lung Needle Biopsy
Sarika Savajiyani MD and Clement U. Singarajah MBBS
Phoenix VA Medical Center
Phoenix, AZ USA
A 67-year-old man with a history of stage IIA rectal adenocarcinoma post neoadjuvant chemoradiation presented with a near code event after elective CT guided biopsy of an enlarging left lower lobe lung nodule. The patient became bradycardic and profoundly hypotensive immediately after the CT guided biopsy with the following vital signs: Systolic BP < 90 mmHg, HR 40/min sinus bradycardia, SpO2 on 100% oxygen non rebreather was 90%. Telemetry and EKG showed ST elevation in the anterior leads. He complained of vague arm and leg weakness and tingling, but did not lose consciousness or suffer a cardiac arrest.
A CT scan was performed about 2-3 minutes after the patient deteriorated (Figure 1).


Figure 1. A-E: Representative images from CT scan in soft tissue windows. Lower: Video of CT scan in soft tissue windows.
What radiographic finding likely explains the patient’s clinical deterioration? (Click on the correct answer to be directed to the second of six pages)
Cite as: Savajiyani S, Singarajah CU. January 2020 critical care case of the month: a code post lung needle biopsy. Southwest J Pulm Crit Care. 2020;20(1):1-6. doi: https://doi.org/10.13175/swjpcc042-19 PDF
Amniotic Fluid Embolism: A Case Study and Literature Review
Ryan J Elsey DO1*, Mary K Moats-Biechler OMS-IV2, Michael W Faust MD3, Jennifer A Cooley CRNA-APRN4, Sheela Ahari MD4, and Douglas T Summerfield MD1
Departments of Internal Medicine1,Obstetrics and Gynecology3,and Anesthesia4
1Mercy Medical Center—North Iowa
Mason City, IA USA
2A.T. Still University
Kirksville, MO USA
Abstract
Amniotic fluid embolus is a rare and life threatening peripartum complication that requires quick recognition and emergent interdisciplinary management to provide the best chance of a positive outcome for the mother and infant. The following case study demonstrates the importance of quick recognition as well as an interdisciplinary approach in caring for such a condition. A literature review regarding the current recommendations for management of this condition follows as well as a proposed treatment algorithm.
Introduction
Amniotic fluid embolus (AFE) is a rare and life-threatening complication of pregnancy; a recent population-based review found an estimated incidence ranging from 1 in 15,200 deliveries in North America and 1 in 53,800 deliveries in Europe (1). Mortality rates vary but have been reported to range from 11% to more than 60%, with the most recent population-based studies in the United States reporting a 21.6% fatality rate (1-4). Despite best efforts, it remains one of the leading causes of maternal death (1,5,6). However, rapid diagnosis of AFE and immediate obstetric and intensive care has proven to play a decisive role in maternal prognosis and survival (7-9).
In 2016, uniform diagnostic criteria were proposed for reporting on cases of AFE. First, a report of AFE requires a sudden onset of cardiorespiratory arrest, which consists of both hypotension (systolic blood pressure < 90 mmHg) and respiratory compromise (dyspnea, cyanosis, or SpO2 < 90%). Secondly, overt disseminated intravascular coagulation (DIC) must be documented following the appearance of signs or symptoms using a standardized scoring system. Coagulopathy must be detected prior to a loss of sufficient blood to account for dilutional or shock-related consumptive coagulopathy. Third, the clinical onset must occur during labor or within 30 minutes of delivery of the placenta. Fourth, no fever ≥ 38.0° C during labor can occur (10).
The following case study qualifies as a reportable incidence of an AFE under the above criteria and further demonstrates the ability to successfully stabilize a patient with AFE due to quick recognition, interdisciplinary cooperation, and effective supportive management.
Case Presentation
A 34-year-old gravida 5, para 1-1-2-2, presented at 36 weeks and 1-day gestation for induction of labor. Her past medical history included esophageal atresia at birth and a past pregnancy complicated by preterm, premature rupture of the membranes. Initial labs at admission were significant for a hemoglobin of 12.2 g/dL and a platelet count of 234 x103 u/L. The patient was subsequently started on lactated ringers at 125 ml/hr. As the patient's labor progressed, an epidural was placed 3 hours after admission. Four hours and 42 minutes after admission, an artificial rupture of the membranes was performed.
Eighteen minutes after the artificial rupture of the membranes was performed, the patient was noted to have seizure-like activity. She was given an intravenous (IV) fluid bolus and ephedrine, and the anesthesia provider was emergently contacted. When anesthesia arrived, the patient was noted to be cyanotic in bed. Patient vitals and exam were significant for emesis, a heart rate of 50 beats per minute (bpm), systolic blood pressure in the low 70s (mmHg), and a fetal heart rate in the 70s.
The differential diagnosis at this time was broad and included anesthesia drug reactions such as an intravascular epidural migration, pulmonary thromboembolism, eclampsia, or even an aortic dissection. A pulmonary embolism was felt to be unlikely due to the patient's bradycardia and sudden neurologic changes. Eclampsia was less likely at the time due to no signs of pre-eclampsia in the patient as well as the patient's current bradycardia and hypotension. Given the patient's absence of Marfan syndrome, aortic dissection was not considered to be a high probability. The patient did have signs consistent with an intravascular epidural including altered mental status, cyanosis, bradycardia, hypotension, vomiting, and a low fetal heart rate. However, at the time anesthesia felt she was more likely suffering from an acute embolic process given the timeframe between the artificial rupture of the membranes and the onset of her symptoms.
Given the patient's instability, she was emergently taken for a cesarean section and intubated to provide airway stabilization. The cesarean section began 15 minutes after seizure like symptoms started and upon delivery, the infant was subsequently transferred to a tertiary center for therapeutic hypothermia.
Intraoperatively, the patient was noted to maintain a peripheral capillary oxygen saturation (SpO2) of >90%. However, end tidal C02 was elevated to 54 mmHg despite hyperventilation and peak airway pressures were elevated to 38 cmH2O. Albuterol and sevoflurane were subsequently utilized in an attempt to increase bronchodilation. Following completion of the caesarian section, peak airway pressures normalized to less than 30 cmH2O but end tidal CO2 levels remained as high as 52 mmHg despite hyperventilation. Blood pressure was significant for systolic pressure of 80 mmHg. IV phenylephrine was administered. Additionally, uterine massage was performed to aid in hemorrhage control and the patient was administered IV oxytocin, methylergonovine maleate, carboprost, and vaginal misoprostol. A repeat complete blood count was performed one hour after symptom onset which showed a hemoglobin of 10.3 g/dL and a platelet count of 103 x103 u/L.
In this case, the patient’s care team had a high suspicion of an AFE with symptoms that followed the uniform diagnostic criteria for an AFE. The patient had hemodynamic instability, coinciding with the recent rupture of membranes. Her systolic blood pressure was < 90 mmHg and her end tidal C02 levels (in mmHg) were elevated to the high 40s and low 50s. The critical care team was notified of her condition and the patient was subsequently transferred to the Intensive Care Unit (ICU) on mechanical ventilation and sedated with fentanyl and versed.
Upon arrival to the ICU, a DIC panel was performed revealing DIC. Labs showed a fibrinogen level of 52 mg/dL, A D-dimer greater than 128,000 ng/mL, and a platelet count of 80,000 u/L despite the administration of one pooled unit of platelets. The patient's international normalized ratio (INR) was 1.3 with a baseline INR of 0.9. Due to multiple laboratory abnormalities and a clinical condition consistent with DIC, aggressive transfusions were performed per the standard of care for patients suffering with DIC. A peripheral smear was obtained revealing schistocytes (Figure 1) which verified the DIC diagnosis.

Figure 1. The patient's peripheral blood smear four hours after onset of symptoms which demonstrates schistocytes indicative of DIC.
Hematology was emergently consulted and it was recommended to avoid additional platelet transfusions unless platelet counts dropped below 10,000 to 20,000 u/L. One milligram (mg) of subcutaneous phytonadione was also given five hours after symptom onset in an effort to decrease bleeding.
Cardiology was consulted and performed an emergent echocardiogram to assess the patient’s heart function and rule out any cardiac abnormalities. Given her past history of esophageal atresia, there was particular concern about an underlying ventricular septal defect, patent ductus arteriosus, or tetralogy of Fallot (11). The echocardiogram revealed a dilated, yet functional right ventricle, which was expected in the setting of an AFE. ICU physicians at a tertiary care center were provisionally consulted to confirm that the patient was a candidate for arteriovenous extracorporeal membrane oxygenation (AV-ECMO) should she suffer further cardiopulmonary collapse. Labs, including hemoglobin, platelets, fibrinogen activity, and ionized calcium were drawn every two hours during the acute phase of the patient's management and abnormalities were addressed as required over the subsequent two hours. The patient's hemoglobin was noted to decline to as low as 6.7 g/dL. Of note, lab draws did suffer some sample lysis due to the patient's coagulation abnormalities. The patient did initially require phenylephrine for blood pressure support. Additionally, she was placed on an experimental septic shock protocol which involved the administration of 1500 mg of ascorbic acid every six hours, 60 mg of methylprednisolone every six hours, and 200 mg of thiamine every 12 hours. The patient began to stabilize around 10 to 12 hours after her AFE symptoms began and pressor support was titrated off, at which point blood draws were liberalized to every four hours. The patient continued to improve and remained stable overnight.
On hospital day two, the patient was noted to be alert and was successfully extubated. Following extubation, the physical exam found her to be neurologically and hemodynamically intact. During her stay in the ICU, the patient received a total of eight units of packed red blood cells, five units of fresh frozen plasma, one pooled unit of platelets, and one unit of cryoprecipitate. The patient was ultimately discharged from the hospital on day four with no long-term sequelae noted.
The patient was informed that data from the case would be submitted for publication and gave her consent.
A Review of the Literature
AFE remains one of the leading causes of direct, maternal mortality among developed countries (1,12,13). Multiple reviews have studied the incidence of AFE, which varies widely, from 1.9 per 100,000 to 7.7 per 100,000 pregnancies, with the reported fatality rate due to AFE ranging from 11% to more than 60%, depending on the study (1,2,4,14). The difficulty in reporting an accurate incidence and fatality rate is likely secondary to the fact that AFE remains a diagnosis of exclusion. AFE is traditionally diagnosed clinically during labor in a woman with ruptured membranes and a triad of symptoms, including unexplained cardiovascular collapse, respiratory distress, and DIC. (1,2,15-18). Additional symptoms may include hypotension, frothing from the mouth, fetal heart rate abnormalities, loss of consciousness, bleeding, uterine atony, and seizure-like activity (15,16,19).
The majority of women who fail to survive an AFE die during the acute phase (median of one hour and 42 minutes after presentation) (2,6). Surviving beyond the acute phase dramatically improves their overall chance of survival; however, survival is not without long term morbidities. Analysis performed in the United Kingdom in 2005 and again in 2015 showed that 7% of woman surviving AFE have permanent neurological injury, including persistent vegetative state/anoxic/hypoxic brain injury or cerebrovascular accident (2,7). Among survivors,17% were shown to have other comorbidities, including sepsis, renal failure, thrombosis or pulmonary edema and 21% required a hysterectomy (2,6).
Despite several decades of research, the pathogenesis of an AFE continues to remain somewhat clouded. Multiple theories have been postulated concerning the clinical manifestations occurring with an AFE and their relationship with the passage of amniotic fluid into the systemic maternal circulation. The first theory proposed described amniotic debris passing through the veins of the endocervix and into maternal circulation, resulting in an obstruction (1,6). This theory has fallen out of favor as there is no physical evidence of obstruction noted on radiologic studies, autopsies, or experimentally in animal models (1,20,21). Additionally, multiple studies have found that that the passage of amniotic and fetal cells into maternal circulation are very common during pregnancy and delivery (6). Thus, most theories today focus on humoral and immunological factors and how they affect the body (5,22,23). Current research focuses on the effect of amniotic fluid on the body after it has already entered into maternal circulation. It is theorized that the amniotic fluid results in the release of various endogenous mediators, resulting in the physiologic changes that are seen with an AFE. Proposed mediators include histamine (22), bradykinin (24), endothelin (25,26), leukotrienes (27), and arachidonic acid metabolites (28).
The hemodynamic response to AFE is biphasic in nature. It consists of vasospasm, resulting in severe pulmonary hypertension, and intense vasoconstriction of the pulmonary vasculature secondary to the amniotic fluid itself, which can lead to ventilation-perfusion mismatch and resultant hypoxia (5,6,29). On an echocardiogram, the initial phase of an AFE consists of right ventricular failure demonstrated by a severely dilated, hypokinetic right ventricle with deviation of the interventricular septum into the left ventricle (18). Following the initial phase of right ventricular failure, which can lasts minutes to hours, left ventricular failure along with cardiogenic, pulmonary edema becomes the prominent finding (1,5). This occurs due to a reduction in preload as well as systemic hypotension. These changes may decrease coronary artery perfusion, which can result in myocardial injury, precipitation of cardiogenic shock, and worsening of distributive shock (1,6,30).
DIC is present in up to 83% of patients experiencing an AFE; however, its onset during presentation can be variable (31). It may present within the first ten minutes following cardiovascular collapse, or it may precipitate up to nine hours following the initial clinical manifestation (5,31,32). The precipitating pathophysiology behind DIC in AFE is poorly understood, but is likely to be consumptive, rather than fibrinolytic, in nature. In an AFE it is currently theorized that tissue factor, which is present in amniotic fluid, activates the extrinsic pathway by binding with factor VII, triggering clotting to occur by activating factor X, resulting in the consumptive coagulopathy (1,33-35). Ultimately, it is felt that this coagulation leads to vasoconstriction of the microvasculature and thrombosis by producing thrombin that is secreted into the endothelin, leading to the changes seen in DIC (1,5,6,14,18).
Recommended Management for AFE Based on Current Literature
Early recognition of AFE and immediate obstetric and intensive care has proven to play a decisive role in maternal prognosis and survival (7,8). In order to survive an an AFE, patients require immediate multidisciplinary management with a focus on maintaining oxygenation, circulatory support, and correcting coagulopathy (1,6).
A literature review of the current management for patients presenting with AFE recommends standard initial lifesaving supportive care. This should begin with immediate protection of the patient's airway via endotracheal intubation and early, sufficient oxygenation using an optimized positive end-expiratory pressure (FiO2:PEEP) ratio, which also decreases the risk of aspiration (1,5,29). Two large bore IV lines should be placed for crystalloid fluid resuscitation. In the setting of a cardiopulmonary arrest, cardiopulmonary resuscitation should be initiated and an immediate caesarian section within three to five minutes should be performed in the presence of a fetus ≥ 23 weeks gestation (5,18,36-38). This serves several purposes, including decreasing the risk of the infant suffering from long term neurologic injury secondary to hypoxia, improving venous flow to the right heart by emptying the uterus, and reducing pressure on the inferior vena cava to decrease impedance to blood flow, which decreases systemic blood pressure (1,5,31,39,40).
During the initial phase, attention should be paid to avoid hypoxia, acidosis, and hypercapnia due to their ability to increase pulmonary vascular resistance and lead to worsening of right heart failure and recommendations include sildenafil, inhaled or injected prostacyclin, and inhaled nitric oxide (6). Recommendations to treat for hypotension during this phase include the utilization of vasopressors, such as norepinephrine or vasopressin (1,6,18,37,41). Hemodynamic management during the second phase should focus on the patient's left-sided heart failure by optimizing cardiac preload via vasopressors to maintain perfusion and utilizing inotropes such as dobutamine or milrinone to increase left ventricular contractility (1,6,18).
Due to the relationship between AFE and DIC, current recommendations suggest early assessment of the patient's coagulation status. Additionally, in the setting of a massive hemorrhage, blood product administration should not be delayed while awaiting laboratory results (18). Early corrective management of the patient's coagulopathy should be aggressive in nature, especially in the setting of a massive hemorrhage. Tranexamic acid and fibrinogen concentrate (for fibrinogen levels below 2 g/L) are essential in the treatment of hyper-fibrinolysis. Additionally, multiple obstetric case studies have shown fibrinogen replacement to benefit from bedside rotational thromboelastometry if available due to its ability to rapidly diagnosis consumptive versus fibrinolytic coagulopathy at the bedside (5,42,43). Hemostatic resuscitation with packed red blood cells, fresh-frozen plasma, and platelets at a ratio of 1:1:1 should be administered (6,18). Cryoprecipitate replacement is recommended as well due to the consumptive nature of DIC in AFE, and its importance should not be understated. A 2015 population-based cohort study showed that women with AFE who died or had permanent neurologic injury were less likely to have received cryoprecipitate than those who survived and were without permanent neurologic injury (1,2). Furthermore, due to the dynamic processes of chemodynamical labs, including hemoglobin, platelet count, and fibrinogen must be monitored closely to prevent complications or over transfusion (14).
Uterine atony is a common feature with AFE and it is recommended to immediately administer uterotonics during the postpartum period to prevent its occurrence (5,44). Should it occur, uterine atony should be managed aggressively via uterotonics such as oxytocin, ergot derivatives, and prostaglandins; refractory cases may require packing material for uterine tamponade, uterine artery ligation, or even a hysterectomy for the most severe (5,8,18).
In addition to the treatments listed above, multiple case reports support the use of aggressive or novel therapeutic modalities to aid in the treatment of AFE; however, for many of the treatments, evidence supporting increased survival of an AFE is merely anecdotal (18). Among the best supported ancillary treatments is nonarterial extracorporeal membrane oxygenation as a possible therapeutic treatment for patients with refractory acute respiratory distress syndrome. However, due to the profoundly coagulopathic state of AFE and the active hemorrhage occurring with AFE, the use of anticoagulation may profoundly worsen bleeding. Consequently, extracorporeal membrane oxygenation is controversial and not routinely recommended in the management of AFE (6,18). Similarly, post-cardiac arrest therapeutic hypothermia with a range of 32°C to 34°C is often avoided in patients with AFE due to the increased risk of hemorrhage given their predisposition for DIC (18). However, in patients not demonstrating DIC and overt bleeding, targeted temperature management to 36°C and preventing hyperthermia is an option that should be considered (17,45,46). Factor VIIa procoagulant, which increases thrombin formation, has been utilized anecdotally, but strong supporting data is lacking; it should only be considered if following the replacement with massive coagulation factors, hemostasis and bleeding fail to improve (5,47). Additionally, it is important to note that factor VIIa replacement is only effective if other clotting factors have been replaced (1,6,48,49). Novel therapeutic modalities mentioned in the literature also include continuous hemofiltration, cardiopulmonary bypass, nitric oxide, steroids, C1 esterase inhibitor concentrate, and plasma exchange transfusion. While there are case reports published to suggest that all of the aforementioned therapies may provide some level of improvement in patients with AFE, the positive results from these cases may be due to their administration during the intermediate phase of AFE as opposed to the acute phase of AFE, where the majority of mortality occurs—once patients have surpassed the early, acute phase, survival chances greatly improve with continued supportive care (1,6).
AFE has traditionally been viewed as a condition associated with poor outcomes and a high mortality rate for both the mother and the infant. However, with quick AFE recognition, high quality supportive care, and interdisciplinary cooperation, patients can have positive outcomes. Based on the success with the patient presented in this case and the review of the current literature as seen above, the authors have proposed an algorithm (Figure 2) for the treatment of future patients experiencing AFE.

Figure 2. Proposed interdisciplinary treatment algorithm for acute management of an AFE.
By following the algorithm, the authors believe that the outcomes for AFE patients can be improved.
Abbreviations
PEEP: positive end-expiratory pressure; BP: blood pressure; TV: tidal volume; ACLS: Advanced cardiac life support; ABG: Arterial blood gas; CBC: Complete blood count; CMP: Complete metabolic profile; INR: International normalized ratio; PTT: Partial prothrombin time; ART line: Arterial line; NO: Nitric oxide; ARDS: Acute respiratory distress syndrome; ECMO: Extracorporeal membrane oxygenation; FFP: Fresh frozen plasma; Plt: Platelet; pRBCs: Packed red blood cells; NE: Norepinephrine.
References
- Conde-Agudelo A, Romero R. Amniotic fluid embolism: an evidence-based review. Am J Obstet Gynecol. 2009;201(5):445-e1. [CrossRef] [PubMed]
- Fitzpatrick D, Tuffnell D, Kurinczuk J, Knight M. Incidence, risk factors, management and outcomes of amniotic-fluid embolism: a population-based cohort and nested case-control study. BJOG. 2016 Jan;123(1):100-9. [CrossRef] [PubMed]
- Cunningham FG, Nelson BD. Disseminated intravascular coagulation syndromes in obstetrics. Obstet Gynecol. 2015;126(5):999-1011. [CrossRef] [PubMed]
- Knight M, Berg C, Brocklehurst P, et al. Amniotic fluid embolism incidence, risk factors and outcomes: a review and recommendations. BMC Pregnancy Childbirth. 2012 Feb 10;12:7. [CrossRef] [PubMed]
- Rath WH, Hofer S, Sinicina I. Amniotic fluid embolism: an interdisciplinary challenge: epidemiology, diagnosis and treatment. Deutsches Ärzteblatt International. 2014;111(8):126. [CrossRef] [PubMed]
- Tuffnell DJ, Slemeck E. Amniotic fluid embolism. Obstetrics,Gynaecology & Reproductive Medicine. 2017;27(3):86-90. [CrossRef]
- Tuffnell D. United Kingdom amniotic fluid embolism register. BJOG. 2005;112(12):1625-9. [CrossRef] [PubMed]
- Matsuda Y, Kamitomo M. Amniotic fluid embolism: a comparison between patients who survived and those who died. J Int Med Res. 2009;37(5):1515-1521. [CrossRef] [PubMed]
- CEMACH. Confidential enquiry into maternal deaths in the United Kingdom,why mothers die 2000-2002. Royal College of Obstetricians and Gynaecologists. 2004.
- Clark SL, Romero R, Dildy GA, et al. Proposed diagnostic criteria for the case definition of amniotic fluid embolism in research studies. Am J Obstet Gynecol. 2016;215(4):408-12. [CrossRef] [PubMed]
- Clark DC. Esophageal atresia and tracheoesophageal fistula. Am Fam Physician. 1999;59(4):910-916,919-20. [PubMed]
- Berg CJ, Callaghan WM, Syverson C, Henderson Z. Pregnancy-related mortality in the United States,1998 to 2005. Obstet Gynecol. 2010;116(6):1302-9. [CrossRef] [PubMed]
- Cantwell R, Clutton-Brock T, Cooper G, et al. Saving Mothers' Lives: Reviewing maternal deaths to make motherhood safer: 2006-2008. The Eighth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG. 2011;118 Suppl 1:1-203. [CrossRef] [PubMed]
- Erez O, Mastrolia SA, Thachil J. Disseminated intravascular coagulation in pregnancy: insights in pathophysiology, diagnosis and management. Am J Obstet Gynecol. 2015;213(4):452-63. [CrossRef] [PubMed]
- Rezai S, Hughes AC, Larsen TB, Fuller PN, Henderson CE. Atypical amniotic fluid embolism managed with a novel therapeutic regimen. Case Rep Obstet Gynecol. 2017;2017:8458375. [CrossRef] [PubMed]
- Clark SL. Amniotic fluid embolism. Obstet Gynecol. 2014;123(2 Pt 1):337-48. [CrossRef] [PubMed]
- Clark SL, Montz FJ, Phelan JP. Hemodynamic alterations associated with amniotic fluid embolism: a reappraisal. Am J Obstet Gynecol. 1985;151(5):617-21. [CrossRef] [PubMed]
- Pacheco LD, Saade G, Hankins GD, Clark SL. Amniotic fluid embolism: diagnosis and management. Am J Obstet Gynecol. 2016;215(2):B16-24. [CrossRef] [PubMed]
- Clark SL. Amniotic fluid embolism. Clin Obstet Gynecol. 2010;53(2):322-8. [CrossRef] [PubMed]
- Stolte L, van Kessel H, Seelen J, Eskes T, Wagatsuma T. Failure to produce thesyndrome of amniotic fluid embolism by infusion of amniotic fluid and meconium into monkeys. Am J Obstet Gynecol. 1967;98(5):694-7. [CrossRef] [PubMed]
- Adamsons K, Mueller-Heubach E, Myers RE. The innocuousness of amniotic fluid infusion in the pregnant rhesus monkey. Am J Obstet Gynecol. 1971;109(7):977-84. [CrossRef] [PubMed]
- Benson MD. A hypothesis regarding complement activation and amniotic fluid embolism. Med Hypotheses. 2007;68(5):1019-25. [CrossRef] [PubMed]
- Benson MD. Current concepts of immunology and diagnosis in amniotic fluid embolism. Clin Dev Immunol. 2012;2012:946576. [CrossRef] [PubMed]
- Robillard J, Gauvin F, Molinaro G, Leduc L, Adam Arrived GE. The syndrome of amniotic fluid embolism: a potential contribution of bradykinin. Am J Obstet Gynecol. 2005;193(4):1508-12. [CrossRef] [PubMed]
- el Maradny Kandalama Halim A, Maehara K, Terao T. Endothelin has a role in early pathogenesis of amniotic fluid embolism. Gynecol Obstet Invest. 1995;40(1):14-8. [CrossRef] [PubMed]
- Khong TY. Expression of endothelin‐1 in amniotic fluid embolism and possible pathophysiological mechanism. BJOG. 1998;105(7):802-4. [CrossRef] [PubMed]
- Azegami Memoria N. Amniotic fluid embolism and leukotrienes. Am J Obstet Gynecol. 1986;155(5):1119-24. [CrossRef] [PubMed]
- Clark SL. Arachidonic acid metabolites and the pathophysiology of amniotic fluid embolism. Semin Reprod Endocrinol. 1985;3:253-7. [CrossRef]
- Stafford I, Sheffield J. Amniotic fluid embolism. Obstet Gynecol Clin North Am. 2007;34(3):545-53,xii. [CrossRef] [PubMed]
- Steiner PE, Lushbaugh CC, Frank HA. Fatal obstetric shock for pulmonary emboli of amniotic fluid. Am J Obstet Gynecol. 1949;58(4):802-5. [CrossRef] [PubMed]
- Clark SL, Hankins GD, Dudley DA, Dildy GA, Porter TF. Amniotic fluid embolism: analysis of the national registry. Am J Obstet Gynecol. 1995;172(4 Pt 1):1158-67; discussion 1167-9. [CrossRef] [PubMed]
- Dean LS, Rogers RP,3rd, Harley RA, Hood DD. Case scenario: amniotic fluid embolism. Anesthesiology. 2012;116(1):186-92. [CrossRef] [PubMed]
- Lockwood CJ, Bach R, Guha A, Zhou XD, Miller WA, Nemerson Y. Amniotic fluid contains tissue factor, a potent initiator of coagulation. Am J Obstet Gynecol.1991;165(5 Pt 1):1335-41. [CrossRef] [PubMed]
- McDougall RJ, Duke GJ. Amniotic fluid embolism syndrome: case report and review. Anaesth Intensive Care. 1995;23(6):735-40. [CrossRef] [PubMed]
- Uszynski M, Zekanowska E, Uszynski W, Kuczynski J. Tissue factor (TF) and tissue factor pathway inhibitor (TFPI) in amniotic fluid and blood plasma: implications for the mechanism of amniotic fluid embolism. Eur J Obstet Gynecol Reprod Biol. 2001;95(2):163-6. [CrossRef] [PubMed]
- Jeejeebhoy FM, Zelop CM, Lipman S, et al. Cardiac Arrest in Pregnancy: A Scientific Statement from the American Heart Association. Circulation. 2015;132(18):1747-73. [CrossRef] [PubMed]
- O'Shea A, Eappen S. Amniotic fluid embolism. Int Anesthesiol Clin. 2007;45(1):17-28. [CrossRef] [PubMed]
- Davies S. Amniotic fluid embolus: a review of the literature. Can J Anaesth. 2001;48(1):88-98. [CrossRef] [PubMed]
- Martin RW. Amniotic fluid embolism. Clin Obstet Gynecol. 1996;39(1):101-6. [CrossRef] [PubMed]
- Martin PS, Leaton MB. Emergency. Amniotic fluid embolism. Am J Nurs. 2001;101(3):43-44. [CrossRef] [PubMed]
- Moore J, Baldisseri MR. Amniotic fluid embolism. Crit Care Med. 2005;33(10 Suppl):S279-285.[CrossRef] [PubMed]
- Collins NF, Bloor M, McDonnell NJ. Hyperfibrinolysis diagnosed by rotational thromboelastometry in a case of suspected amniotic fluid embolism. Int J Obstet Anesth. 2013;22(1):71-6. [CrossRef] [PubMed]
- Loughran JA, Kitchen TL, Sindhaker S, Ashraf M, Awad M, Kealaher EJ. Rotational thromboelastometry (ROTEM®)-guided diagnosis and management of amniotic fluid embolism. Int J Obstet Anesth. 2018. Sep 11. pii: S0959-289X(18)30122-5. [CrossRef] [PubMed]
- Tuffnell D, Knight M, Plaat F. Amniotic fluid embolism - an update. Anaesthesia. 2011;66(1):3-6. [CrossRef] [PubMed]
- Nielsen N, Wetterslev J, Cronberg T, et al. Targeted temperature management at 33 C versus 36 C after cardiac arrest. N Engl J Med. 2013;369(23):2197-206. [CrossRef] [PubMed]
- Callaway CW, Donnino MW, Fink EL, et al. Part 8: Post-cardiac arrest care: 2015 American Heart Association Guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 Suppl 2):S465-82. [CrossRef] [PubMed]
- Leighton BL, Wall MH, Lockhart EM, Phillips LE, Zatta AJ. Use of recombinant factor VIIa in patients with amniotic fluid embolism: a systematic review of case reports. Anesthesiology. 2011;115(6):1201-8. [CrossRef] [PubMed]
- Prosper SC, Goudge CS, Lupo VR. Recombinant factor VIIa after amniotic fluid embolism and disseminated intravascular coagulopathy. Obstet Gynecol. 2007;109(2 pt 2):524-5. [CrossRef] [PubMed]
- Lim Y, Loo CC, Chia V, Fun W. Recombinant factor VIIa after amniotic fluid embolism and disseminated intravascular coagulopathy. Int J Gynaecol Obstet. 2004;87(2):178-9. [CrossRef] [PubMed]
Cite as: Elsey RJ, Moats-Biechler MK, Faust MW, Cooley JA, Ahari S, Summerfield DT. Amniotic fluid embolism: A case study and literature review. Southwest J Pulm Crit Care. 2019;18(4):94-105. doi: https://doi.org/10.13175/swjpcc105-18 PDF
Ultrasound for Critical Care Physicians: Caught in the Act
Uzoamaka Ogbonnah MD1
Isaac Tawil MD2
Trenton C. Wray MD2
Michel Boivin MD1
1Department of Internal Medicine
2Department of Emergency Medicine
University of New Mexico School of Medicine
Albuquerque, NM USA
A 16-year-old man was brought to the Emergency Department via ambulance after a fall from significant height. On arrival to the trauma bay, the patient was found to be comatose and hypotensive with a blood pressure of 72/41 mm/Hg. He was immediately intubated, started on norepinephrine drip with intermittent dosing of phenylephrine, and transfused with 3 units of packed red blood cells. He was subsequently found to have extensive fractures involving the skull and vertebrae at cervical and thoracic levels, multi-compartmental intracranial hemorrhages and dissection of the right cervical internal carotid and vertebral arteries. He was transferred to the intensive care unit for further management of hypoxic respiratory failure, neurogenic shock and severe traumatic brain injury. Following admission, the patient continued to deteriorate and was ultimately declared brain dead 3 days later. The patient’s family opted to make him an organ donor
On ICU day 4, one day after declaration of brain death, while awaiting organ procurement, the patient suddenly developed sudden onset of hypoxemia and hypotension while being ventilated. The patient had a previous trans-esophageal echo (TEE) the day prior (Video 1). A repeat bedside TEE was performed revealing the following image (Video 2).

Video 1. Mid-esophageal four chamber view of the right and left ventricle PRIOR to onset of hypoxemia.

Video 2. Mid-esophageal four chamber view of the right and left ventricle AFTER deterioration.
What is the cause of the patient’s sudden respiratory deterioration? (Click on the correct answer to be directed to an explanation)
- Atrial Myxoma
- Fat emboli syndrome
- Thrombus in-transit and pulmonary emboli
- Tricuspid valve endocarditis
Cite as: Ogbonnah U, Tawil I, Wray TC, Boivin M. Ultrasound for critical care physicians: Caught in the act. Southwest J Pulm Crit Care. 2018;17(1):36-8. doi: https://doi.org/10.13175/swjpcc091-18 PDF
June 2018 Critical Care Case of the Month
Stephanie Fountain, MD
Banner University Medical Center Phoenix
Phoenix, AZ USA
History of Present Illness
A 60-year-old native American man presented to an outside hospital with several days of nausea, vomiting and diarrhea. The patient felt weak and called emergency medical services and was taken to the emergency department.
Past Medical History
He has a history of end stage renal disease secondary to diabetes mellitus and hypertension. He received a cadaveric renal transplant in 2008 which was complicated with acute on chronic rejection and symptomatic hyponatremia.
Physical Examination
His pulse was recorded as 28 beats/min and his blood pressure was 90/60.
Which of the following should be done? (Click on the correct answer to be directed to the second of six pages)
Cite as: Fountain S. June 2018 critical care case of the month. Southwest J Pulm Crit Care. 2018;16(6):304-10. doi: http://doi.org/10.13175/swjpcc065-18 PDF
Fatal Consequences of Synergistic Anticoagulation
Payal Sen, MD1
Uddalak Majumdar, MD2
Patrick Rendon, MD1
Ali Imran Saeed, MD1
Akshay Sood, MD1
Michel Boivin, MD1
1University of New Mexico
Albuquerque, NM US
2Cleveland Clinic Foundation
Cleveland, OH USA
Abstract
Objective: Novel oral anticoagulants (NOACs) are increasingly being preferred by clinicians (and patients) because they have a wide therapeutic window and therefore do not require monitoring of anticoagulant effect. Herein, we describe the unfortunate case of a patient who had fatal consequences as a result of switching from warfarin to rivaroxaban.
Case Summary: A 90-year-old Caucasian woman, with atrial fibrillation on chronic anticoagulation with warfarin, was admitted to the hospital for pneumonia. She was treated with levofloxacin. In the same admission, her warfarin was switched to rivaroxaban. On Day 3 after the switch, her INR was found to be 6, and she developed a cervical epidural hematoma from C2 to C7. She ultimately developed respiratory arrest, was put on comfort care and died.
Discussion: Rivaroxaban and warfarin are known to have a synergistic anticoagulant effect, usually seen shortly after switching. Antibiotics also increase the effects of warfarin by the inhibition of metabolizing isoenzymes. It is hypothesized that these two effects led to the fatal cervical spinal hematoma.
Conclusion: The convenience of a wide therapeutic window and no requirement of laboratory monitoring makes the NOACs a desirable option for anticoagulation. However, there is lack of data and recommendations on how to transition patients from Warfarin to NOACs or even how to transition from one NOAC to another. Care should be taken to ensure continuous monitoring of anticoagulation when stopping, interrupting or switching between NOACS to avoid the possibility of fatal bleeding and strokes.
Introduction
Novel oral anticoagulants (NOACs) are increasingly being preferred by clinicians (and patients) because they have a wide therapeutic window and therefore do not require monitoring of anticoagulant effect. They have also shown greater efficacy and safety when compared to warfarin (1). The choice among the novel oral anticoagulants depends on their different pharmacokinetic profile, patients' stroke and bleeding risk, comorbidities, drug tolerability and costs and, finally, patients' preferences (2). There is however, paucity of evidence regarding the process of switching from warfarin to a NOAC, from one NOAC to the other, and the consequent ‘synergism’ (3). Herein, we describe the unfortunate case of a patient who had fatal consequences as a result of switching from warfarin to rivaroxaban. We also wish to highlight the adverse effects that antibiotic interaction can have with both warfarin and the NOACS (4).
Case Report
A 90-year-old Caucasian woman, who resided in a nursing home was admitted to the hospital with chief complaints of fever and confusion for 2 days. She also had intermittent cough, but denied headache, blurry vision, dysuria, diarrhea and constipation. Past medical history was significant for non-valvular atrial fibrillation, for which she was on therapeutic anticoagulation with warfarin. Family history and social history were not significant. Vitals revealed a temperature of 100 F and physical exam was positive for crackles in the right lower lobe of the lung. Her white count was elevated at 16 x 103/µL, and hepatic and renal function were both normal. Chest x-ray revealed a right sided lower lobe pneumonia. She was admitted to the hospital for acute metabolic encephalopathy due to sepsis secondary to hospital associated pneumonia and was initially given a dose of vancomycin and piperacillin tazobactam, which was later narrowed to levofloxacin.
Hospital Course
On day 2, the patient’s disorientation had improved marginally and her white count had also reduced to 11. Her INR was therapeutic on warfarin and she underwent transesophageal echocardiography and cardioversion for symptomatic atrial fibrillation with rapid ventricular rate. After a long discussion with the patient and her family, it was decided to switch from warfarin to rivaroxaban, to avoid the hassle of frequent INR monitoring.
On Day 3, the patient suddenly developed tachypnea, hypotension and dysarthria after receiving the second dose of rivaroxaban. Rapid Response had to be called. Vitals revealed blood pressure of 92/52, respiratory rate 20, and heart rate of 84 with pulse oximetry showing 92% on 2 liters nasal cannula.
Neurological Examination
Cognition was relatively normal. Patient was alert and oriented X 3.
Motor exam: The patient was quadriplegic.
Touch, pain, and pressure sensations were absent (0/4) below C3-C4.
Reflexes were diminished (¼) and she had absolutely no feeling of any noxious stimuli. Babinsky' s sign was negative.
Urgent Labs on Day 3 (current day)
Arterial blood gases: PaO2 of 62 on 3 liters oxygen via Nasal cannula, PaCO2 of 78.
International Normalized Ratio (INR): 6, prothrombin time was 64.2 seconds.
Radiographic Imaging

Figure 1. Computed tomography scan of the neck revealed posterior cervical epidural hematoma (arrow) from C2 to C7 with cord compression.

Figure 2. Posterior epidural hematoma (arrow) extending from C2-3 through approximately C6-7, which caused significant spinal stenosis.
The patient was then rushed to the neurosurgical ICU. Neurosurgery was consulted and recommended reversing the anticoagulation and taking the patient for emergency surgical evacuation of the hematoma. However, on further discussion with the family, it was revealed that the patient’s earlier wishes had been to never be bedbound and paralyzed. Since she was a 90-year-old patient, chronically debilitated, with a do not resuscitate code status, the ultimate decision was to place her on comfort care. Patient passed away 24 hours later.
Discussion
Rivaroxaban and warfarin are known to have a synergistic anticoagulant effect, usually seen shortly after switching (5). Antibiotics also increase the effects of warfarin by the inhibition of metabolizing isoenzymes (4). It is hypothesized that these two effects led to the fatal cervical spinal hematoma.
For decades, vitamin K antagonists like warfarin have been the agent of choice for oral anticoagulation in different clinical conditions. However, the disadvantages of warfarin are that it needs frequent INR monitoring, has a narrow therapeutic window and interacts with multiple food substances and drugs (6). Warfarin is also known to cause major bleeding. The NOACS (novel oral anticoagulants) such as the direct thrombin inhibitor dabigatran, and Factor Xa Inhibitors like rivaroxaban, edoxaban and apixaban have been developed almost fifty years after the approval of warfarin (7). These NOACS have more predictable pharmacodynamics and pharmacokinetics, fewer drug and dietary interactions and have the added advantage of not requiring frequent laboratory monitoring (7,8). Clinicians are increasingly using these NOACS to replace Vitamin K antagonists for multiple indications like the prevention of thromboembolic complications in atrial fibrillation, treatment of Deep vein thrombosis (DVT) and pulmonary embolism (PE), and thromboprophylaxis during orthopedic surgery (9).
Rivaroxaban, which is an oxazolidinone derivative, inhibits both free Factor Xa and Factor Xa bound in the prothrombinase complex (10). It is a highly selective Factor Xa inhibitor and has high oral bioavailability, with rapid onset of action and a predictable pharmacokinetic profile across a wide spectrum of patients with respect to gender, age, weight and race (11). There is paucity of data on how to safely switch from warfarin to rivaroxaban. Expert opinion is to switch 24 hours after INR < 3 (3). There is only one observational matched-cohort study of switching from warfarin to rivaroxaban and results supported present practices (3). It analyzed a French registry and fluindidione (not warfarin) was the Vitamin K Antagonist in about 90% of the study subjects. In another study of in silico effects, a post-switch synergistic anticoagulant effect has also been observed and a nomogram has been developed for switching to Rivaroxaban, based on INR for Caucasian and Japanese patients (5). INR is affected variably by rivaroxaban and cannot be used as a marker for its anticoagulant effect (12). Laboratory monitoring of anticoagulant effect of NOACs needs to be considered, since INR is unsuitable for this (13).
Some of the manufacturers offer guidance relating to switching from warfarin to NOACs:
- To apixaban: warfarin should be discontinued and apixaban started when the INR is <2.0.
- To dabigatran: warfarin should be discontinued and dabigatran started when the INR is <2.0.
- To rivaroxaban: warfarin should be discontinued and rivaroxaban started when the INR is <3.0.
With longer experience with these NOACs in Europe, the European Heart Rhythm Association does make slightly different recommendations than those in the United States (14). Again, looking at switching from a vitamin K antagonist to a NOAC, the group suggests:
- The NOAC can be immediately initiated once the INR is <2.0.
- If the INR is 2.0 to 2.5, the NOAC can be started immediately or (preferably) the next day.
- If the INR is >2.5, use agent pharmacokinetics to estimate the time for the next INR.
As for moving from parenteral anticoagulation to a NOAC, the European recommendation is:
- For unfractionated heparin (UFH), start the NOAC once the UHF is discontinued.
- For low-molecular weight heparin (LMWH), start the NOAC when the next dose of LMWH would have been due.
Hence, switching vitamin K antagonists to newer direct oral anticoagulants (NOACs) is becoming routine now, since the latter are thought to have a reduced incidence of intracranial bleeding (15). This case teaches us that the synergistic effect and interactions with antibiotics should be kept in mind during switching and when possible, nomograms should be used. Further study is required regarding bridging doses, bridging periods and population-specific dosing.
Conclusion
The convenience of a wide therapeutic window and no requirement of laboratory monitoring makes the NOACs a desirable option for anticoagulation. However, there is lack of data and recommendations on how to transition patients from a vitamin K antagonist to NOACs or even how to transition from one NOAC to another. Care should be taken to ensure continuous monitoring of anticoagulation when stopping, interrupting or switching between NOACS to avoid the possibility of fatal bleeding and strokes. Further trials are also needed to test for appropriate laboratory monitoring of the NOACs. Also, caution must be used whilst using antibiotics with the NOACs, since their interaction can often increase the efficacy of the NOACs and lead to fatal bleeding, like in our patient.
References
- Prisco D, Cenci C, Silvestri E, Ciucciarelli L, Di Minno G. Novel oral anticoagulants in atrial fibrillation: which novel oral anticoagulant for which patient? J Cardiovasc Med (Hagerstown). 2015 Jul;16(7):512-9. [CrossRef] [PubMed]
- Gallego P, Roldan V, Lip GY. Novel oral anticoagulants in cardiovascular disease. J Cardiovasc Pharmacol Ther. 2014 Jan;19(1):34-44. [CrossRef] [PubMed]
- Bouillon K, Bertrand M, Maura G, Blotiere PO, Ricordeau P, Zureik M. Risk of bleeding and arterial thromboembolism in patients with non-valvular atrial fibrillation either maintained on a vitamin K antagonist or switched to a non-vitamin K-antagonist oral anticoagulant: a retrospective, matched-cohort study. Lancet Haematol. 2015 Apr;2(4):e150-9. [CrossRef] [PubMed]
- Lane MA, Zeringue A, McDonald JR. Serious bleeding events due to warfarin and antibiotic coprescription in a cohort of veterans. Am J Med. 2014 Jul;127(7):657-663.e2. [CrossRef] [PubMed]
- Burghaus R, Coboeken K, Gaub T, Niederalt C, Sensse A, Siegmund HU, Weiss W, Mueck W, Tanigawa T, Lippert J. Computational investigation of potential dosing schedules for a switch of medication from warfarin to rivaroxaban-an oral, direct Factor Xa inhibitor. Front Physiol. 2014 Nov 7;5:417. [CrossRef] [PubMed]
- Ezekowitz MD, Aikens TH, Brown A, Ellis Z. The evolving field of stroke prevention in patients with atrial fibrillation. Stroke. 2010 Oct;41(10 Suppl):S17-20. [CrossRef] [PubMed]
- Mendell J, Zahir H, Matsushima N, Noveck R, Lee F, Chen S, Zhang G, Shi M. Drug-drug interaction studies of cardiovascular drugs involving P-glycoprotein, an efflux transporter, on the pharmacokinetics of edoxaban, an oral factor Xa inhibitor. Am J Cardiovasc Drugs. 2013 Oct;13(5):331-42. [CrossRef] [PubMed]
- Ogata K, Mendell-Harary J, Tachibana M, Masumoto H, Oguma T, Kojima M, Kunitada S. Clinical safety, tolerability, pharmacokinetics, and pharmacodynamics of the novel factor Xa inhibitor edoxaban in healthy volunteers. J Clin Pharmacol. 2010 Jul;50(7):743-53. [CrossRef] [PubMed]
- Bauer KA. Recent progress in anticoagulant therapy: oral direct inhibitors of thrombin and factor Xa. J Thromb Haemost. 2011 Jul;9 Suppl 1:12-9. [CrossRef] [PubMed]
- Roehrig S, Straub A, Pohlmann J, Lampe T, Pernerstorfer J, Schlemmer KH, Reinemer P, Perzborn E. Discovery of the novel antithrombotic agent 5-chloro-N-({(5S)-2-oxo-3- [4-(3-oxomorpholin-4-yl)phenyl]-1,3-oxazolidin-5yl}methyl)thiophene- 2-carboxamide (BAY 59-7939): an oral, direct factor Xa inhibitor. J Med Chem. 2005 Sep 22;48(19):5900-8. [CrossRef] [PubMed]
- Eriksson BI, Borris LC, Dahl OE, Haas S, Huisman MV, Kakkar AK, Muehlhofer E, Dierig C, Misselwitz F, Kälebo P; ODIXa-HIP Study Investigators. A once-daily, oral, direct Factor Xa inhibitor, rivaroxaban (BAY 59-7939), for thromboprophylaxis after total hip replacement. Circulation. 2006 Nov 28;114(22):2374-81. [CrossRef] [PubMed]
- Favaloro EJ, Lippi G. The new oral anticoagulants and the future of haemostasis laboratory testing. Biochem Med (Zagreb). 2012;22(3):329-41. [CrossRef] [PubMed]
- Lindahl TL, Baghaei F, Blixter IF, Gustafsson KM, Stigendal L, Sten-Linder M, Strandberg K, Hillarp A; Expert Group on Coagulation of the External Quality Assurance in Laboratory Medicine in Sweden. Effects of the oral, direct thrombin inhibitor dabigatran on five common coagulation assays. Thromb Haemost. 2011 Feb;105(2):371-8. [CrossRef] [PubMed]
- Heidbuchel H, Verhamme P, Alings M, Antz M, Hacke W, Oldgren J, Sinnaeve P, Camm AJ, Kirchhof P; European Heart Rhythm Association. European Heart Rhythm Association Practical Guide on the use of new oral anticoagulants in patients with non-valvular atrial fibrillation. Europace. 2013 May;15(5):625-51. [CrossRef] [PubMed]
- Caldeira D, Barra M, Pinto FJ, Ferreira JJ, Costa J. Intracranial hemorrhage risk with the new oral anticoagulants: a systematic review and meta-analysis. J Neurol. 2015 Mar;262(3):516-22. [CrossRef] [PubMed]
Cite as: Sen P, Majumdar U, Rendon P, Saeed AI, Sood A, Boivin M. Fatal consequences of synergistic anticoagulation. Southwest J Pulm Crit Care. 2018;16(5):289-95. doi: https://doi.org/10.13175/swjpcc058-18 PDF
May 2018 Critical Care Case of the Month
Lacey Gagnon APRN, CNP
Theo Loftsgard APRN, CNP
Department of Anesthesiology and Critical Care
Mayo Clinic Minnesota
Rochester, MN USA
Chief Complaint
Shortness of breath
History of Present Illness
The patient is a 44-year-old woman who was admitted with a history of “pericarditis”. She has a several years history of progressive shortness of breath, abdominal distention and lower extremity edema.
Past Medical History, Social History and Family History
She has a history of obesity, poorly controlled type 2 diabetes, uterine fibroids and hypertension. She does not smoke but does have 1-2 alcoholic beverages per day. Family history is noncontributory.
Physical Examination
- Vital signs: pulse 96 beats/min, blood pressure 110/85 mm Hg, temperature 37° C, respirations 18 breaths/min.
- Neck: there is jugular venous distention with a positive hepatojugular reflux.
- Lungs: rales at both bases.
- Heart: regular rhythm without murmur.
- Abdomen: Distended. Shifting dullness is present.
- Extremities: 2-3 pretibial pitting edema.
Chest Radiography
Chest x-ray shows a small right pleural effusion with mild vascular congestion at the bases. Heart size is normal.
Which of the following should be performed?
Cite as: Gagnon L, Loftsgard T. May 2018 critical care case of the month. Southwest J Pulm Crit Care. 2018;16(5):245-51. doi: https://doi.org/10.13175/swjpcc048-18 PDF
August 2017 Critical Care Case of the Month
Kolene E. Bailey, MD1
Carolyn Welsh, MD1,2
Pulmonary Sciences and Critical Care Medicine
1University of Colorado Anschutz Medical Campus and 2VA Eastern Colorado Health Care System
Denver, CO USA
History of Present Illness
The patient is a 26-year-old woman with who was admitted to the hospital for second cycle of chemotherapy for a large mediastinal synovial sarcoma diagnosed 2 months prior to admission. Symptoms started 6 months prior to presentation with cough. She related the cough to her cigarette smoking and quit. Upon persistence of symptoms, she was evaluated by her physician who ordered imaging. Work-up revealed a large 12 x 14cm synovial sarcoma with internal necrosis that encased the subclavian artery, and descending thoracic aorta, inseparable from pericardium and left atrium. It also encased the pulmonary veins, pulmonary arteries, and airways. Malignancy was complicated by extensive left upper extremity DVT for which she has been on anticoagulation since her last admission, SVC syndrome, and severe mucositis.
Past Medical History, Family History, and Social History
She has a past medical history significant for malignant melanoma surgically resected 7 years previously, as well as generalized an anxiety disorder.
Her family history includes a maternal grandfather with esophageal cancer and maternal great-grandmother with pancreatic cancer. She is single and lives with her parents. She is a former 8 pack year smoker, and daily edible marijuana user. She worked as a hairdresser, but is now unable to work.
Current Medications:
- Escitalopram (Lexapro) 10mg PO daily
- Dalteparin
- Oxycontin 10mg PO BID + Oxycodone 5-10mg PO Q4H PRN pain
- Antiemetics: Compazine PRN, Ondansetron PRN, dexamethasone 4mg BID for 3 days following chemotherapy
- Lorazepam 1mg PO Q4H PRN anxiety
- Pegfilgastrim after chemotherapy
- Senna 3 tabs in AM, 2 tabs in PM
Hospital Course
After starting cycle #2 of chemotherapy (doxorubicin, ifosfamide, and mesna), she experienced significant nausea and anxiety and was prescribed scheduled ondansetron/dexamethasone, prochlorperazine, promethazine and lorazepam. The night of hospital day #2, her providers noticed altered mental status and unusual behavior. They asked her draw a clock which is shown (Figure 1).

Figure 1. Clock drawn by patient.
What is on your differential diagnosis for this patient’s altered mental status? (Click on the correct answer to proceed to the second of five pages)
- Delirium
- Ifosfamide-induced encephalopathy
- Toxic-metabolic encephalopathy secondary to the medications received
- 1 and 3
- All of the above
Cite as: Bailey KE, Welsh C. August 2017 critical care case of the month. Southwest J Pulm Crit Care. 2017;15(2):61-6. doi: https://doi.org/10.13175/swjpcc094-17 PDF
January 2017 Critical Care Case of the Month
Seth Assar, MD
Clement U. Singarajah, MD
Pulmonary and Critical Care Medicine
Banner University Medical Center Phoenix – Phoenix
Phoenix VA Medical Center
Phoenix, AZ USA
History of Present Illness
The patient is a 48-year-old man who presented with two days of progressive shortness of breath and non-productive cough. There were no associated symptoms and the patient specifically denied fever, chills, night sweats, myalgia or other evidence of viral prodrome. He had no chest pain or tightness, nausea, vomiting, or leg swelling and he could lay flat. He had no recent travel or sick contacts and was Influenza-immunized this season.
Past Medical History
- Hypertension
- Hyperlipidemia
- Type 2 diabetes mellitus with a recent hemoglobin A1C of 11%
Social History
- Cook at pizzeria
- Gay and lives at home with roommate of several years
- Smokes marijuana weekly.
- Prior history of cocaine use
Family History
- Noncontributory
Physical Examination
- Vitals: T 99.1º F / HR 125 / BP 193/93 / RR 24 / SpO2 88%
- General: Tachypneic. Alert and oriented X 4.
- Lungs: Crackles at bases bilaterally, no wheezes
- Heart: tachycardia
- Abdomen: NSA
- Skin: no needle marks or cellulitis
Laboratory
- CBC: WBC 11,700 cells/mcL with 80% polymorphonuclear leukocytes, otherwise normal
- Basic metabolic panel: normal
- Brain natriuretic peptide: 120 pg/ml
- Urine drug screen was negative for cocaine but positive for marijuana.
- D-dimer: 0.32 mcg/mL
Hospital Course
He was admitted to the ICU but quickly deteriorated and was intubated for hypoxemia. Empiric ceftriaxone and levofloxacin were begun.
Chest x-ray demonstrated bilateral patchy airspace opacities (Figure 1).

Figure 1. Admission chest x-ray.
Which of the following should be done next? (click on the correct answer to proceed to the second of six pages)
- Bedside cardiac ultrasound
- Coccidioidomycosis serology
- CT scan of the chest
- 1 and 3
- All of the above
Cite as: Assar S, Singarajah CU. January 2017 critical care case of the month. Southwest J Pulm Crit Care. 2017;14(1):6-13. doi: https://doi.org/10.13175/swjpcc143-16 PDF
Ultrasound for Critical Care Physicians: A Pericardial Effusion of Uncertain Significance
Brandon Murguia M.D.
Department of Medicine
University of New Mexico School of Medicine
Albuquerque, NM USA
A 75-year-old woman with known systolic congestive heart failure (ejection fraction of 40%), chronic atrial fibrillation on rivaroxaban oral anticoagulation, morbid obesity, and chronic kidney disease stage 3, was transferred to the Medical Intensive Care Unit for acute hypoxic respiratory failure thought to be secondary to worsening pneumonia.
She had presented to the emergency department 3 days prior with shortness of breath, malaise, left-sided chest pain, and mildly-productive cough over a period of 4 days. She had mild tachycardia on presentation, but was normotensive without tachypnea, hypoxia, or fever. Routine labs were remarkable for a leukocytosis of 15,000 cells/μL. Cardiac biomarkers were normal, and electrocardiogram demonstrated atrial fibrillation with rapid ventricular rate of 114 bpm. Chest x-ray revealed cardiomegaly and left lower lobe consolidation consistent with bacterial pneumonia. Patient was admitted to the floor for intravenous antibiotics, cardiac monitoring, and judicious isotonic fluids if needed.
On night 2 of hospitalization, the patient developed respiratory distress with tachypnea, pulse oximetry of 80-85%, and increased ventricular response into the 140 bpm range. The patient remained normotensive. A portable anterior-posterior chest x-ray showed cardiomegaly and now complete opacification of the left lower lobe. She was transferred to the MICU for suspected worsening pneumonia and congestive heart failure.
Upon arrival to the intensive care unit, vital signs were unchanged and high-flow nasal cannula was started at 6 liters per minute. A focused point-of-care cardiac ultrasound (PCU) was done, limited in quality by patient body habitus, but nonetheless demonstrating the clear presence of a moderate pericardial effusion on subcostal long axis view.

Figure 1: Subcostal long axis view of the heart.
What should be done next regarding this pericardial effusion? (Click on the correct answer for the answer and explanation)
- Observe, this is not significant.
- Additional echocardiographic imaging /evaluation.
- Immediate pericardiocentesis.
- Fluid challenge.
Cite as: Murguia B. Ultrasound for critical care physicians: a pericardial effusion of uncertain significance. Southwest J Pulm Crit Care. 2016;13(5):261-5. doi: https://doi.org/10.13175/swjpcc127-16 PDF
November 2016 Critical Care Case of the Month
Richard A. Robbins, MD
Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ USA
History of Present Illness
A 45-year-old Iraqi War Veteran was seen in the outpatient clinic after referral for COPD based on abnormal blood gases. He denies any dyspnea or cough.
PMH, SH and FH
He has a history of a lower back injury and uses a motorized wheelchair. His pain is managed with morphine sulfate ER 60 mg daily and morphine sulfate 10 mg every 4 hours as needed for breakthrough pain.
He does not smoke cigarettes but does use marijuana for pain. He denies alcohol abuse.
Physical Examination
Physical examination shows a lethargic man in a wheelchair who intermittently falls asleep during questioning and examination. When aroused he is oriented to time, place and person and frequently mentions that his pain is a 10. His vital signs are normal expect his SpO2 is 75% on room air. His lungs were clear and his heart had a regular rhythm without murmur. His pupil size is approximately 2 mm bilaterally and muscle strength is difficult to determine due to his inability to remain alert or fully cooperate.
Radiography
A chest x-ray had been performed about a week previously (Figure 1).

Figure 1. Initial chest x-ray.
Spirometry had been performed earlier in the day (Figure 2).

Figure 2. Spirometry.
Which of the following are indicated at this time? (Click on the correct answer to proceed to the second of four pages)
- Arterial blood gases (ABGs)
- Immediate intubation
- Intensive care unit (ICU) admission
- 1 and 3
- All of the above
Cite as: Robbins Ra. November 2016 critical care case of the month. Southwest J Pulm Crit Care. 2016;13(5):196-201. doi: http://dx.doi.org/10.13175/swjpcc103-16 PDF
Ultrasound for Critical Care Physicians: Unraveling a Rapid Drop of Hematocrit
Deepti Baheti, MBBS
Pablo Garcia, MD
Department of Internal Medicine and LifeBridge Critical Care
Sinai Hospital of Baltimore.
Baltimore, MD USA
An 85-year-old woman was admitted to our hospital with complaints of shortness of breath on exertion. Her medical history was significant for hypertension, pulmonary embolism and stage III chronic kidney disease. She was diagnosed with severe decompensated pulmonary hypertension and started to improve with diuretics. While hospitalized, she suffered an asystolic arrest and was successfully resuscitated. As a result of chest compressions, the patient developed multiple anterior rib fractures. Within a few days of recovering from her cardiac arrest, she was anticoagulated with enoxaparin as a bridge to warfarin for her prior history of pulmonary embolism. Five days after initiation of enoxaparin and warfarin, she was noted to have an acute drop in her hemoglobin from 8 g/dl to 5 g/dl. A thorough physical examination revealed a large area of swelling in her left anterior chest wall. Point-of- care ultrasound was utilized to image this area of swelling centered at the 3rd intercostal space between the mid-clavicular and anterior axillary line (Figures 1 and 2).

Figure 1. Ultrasound image of the chest wall in the sagittal plane.

Figure 2. Ultrasound image of the chest wall in the transverse plane.
What is the cause of this patient’s acute anemia? (Click on the correct answer for an explanation)
Cite as: Baheti D, Garcia P. Ultrasound for critical care physicians: unraveling a rapid drop of hematocrit. Southwest J Pulm Crit Care. 2016;13(2):84-7. doi: http://dx.doi.org/10.13175/swjpcc078-16 PDF
Ultrasound for Critical Care Physicians: Complication of a Distant Malignancy
S. Cham Sante M.D.1
Michel Boivin M.D.2
Department of Emergency Medicine1
Division of Pulmonary, Critical care and Sleep Medicine2
University of New Mexico School of Medicine
Albuquerque, NM USA
An 82-year-old woman with prior medical history of stage IV colon cancer and chronic obstructive pulmonary disease presented to the medical intensive care unit with newly diagnosed community acquired pneumonia and acute kidney injury. The patient presented with acute onset of shortness of breath, nausea, generalized weakness, bilateral lower extremity swelling and decreased urine output. She was transferred for short term dialysis in the setting of multiple electrolyte abnormalities, including hyperkalemia of 6.4 mmol/l, as well as a creatinine of 6.5 mg/dl. The following imaging of the right internal jugular vein was performed with ultrasound during preparation for placement of a temporary triple lumen hemodialysis catheter.

Figure 1. Panel A: Transverse ultrasound image of the right neck. Panel B: Longitudinal ultrasound image of the right neck, centered on the internal jugular vein.
Based on the above imaging what would be the best location to place the dialysis catheter? (Click on the correct answer for an explanation and discussion)
Cite as: Sante SC, Boivin M. Ultrasound for critical care physicians: complication of a distant malignancy. Southwest J Pulm Crit Care. 2016;13(1):27-9. doi: http://dx.doi.org/10.13175/swjpcc055-16 PDF
March 2016 Critical Care Case of the Month
Theo Loftsgard APRN, ACNP
Joel Hammill APRN, CNP
Mayo Clinic Minnesota
Rochester, MN USA
Critical Care Case of the Month CME Information
Members of the Arizona, New Mexico, Colorado and California Thoracic Societies and the Mayo Clinic are able to receive 0.25 AMA PRA Category 1 Credits™ for each case they complete. Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Theo Loftsgard APRN, ACNP. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives:
As a result of this activity I will be better able to:
- Correctly interpret and identify clinical practices supported by the highest quality available evidence.
- Will be better able to establsh the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Will improve the translation of the most current clinical information into the delivery of high quality care for patients.
- Will integrate new treatment options in discussing available treatment alternatives for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine
Current Approval Period: January 1, 2015-December 31, 2016
Financial Support Received: None
History of Present Illness
A 58-year-old man was admitted to the ICU in stable condition after an aortic valve replacement with a mechanical valve.
Past Medical History
He had with past medical history significant for endocarditis, severe aortic regurgitation related to aortic valve perforation, mild to moderate mitral valve regurgitation, atrial fibrillation, depression, hypertension, hyperlipidemia, obesity, and previous cervical spine surgery. As part of his preop workup, he had a cardiac catheterization performed which showed no significant coronary artery disease. Pulmonary function tests showed an FEV1 of 55% predicted and a FEV1/FVC ratio of 65% consistent with moderate obstruction.
Medications
Amiodarone 400 mg bid, digoxin 250 mcg, furosemide 20 mg IV bid, metoprolol 12.5 mg bid. Heparin nomogram since arrival in the ICU.
Physical Examination
He was extubated shortly after arrival in the ICU. Vitals signs were stable. His weight had increased 3 Kg compared to admission. He was awake and alert. Cardiac rhythm was irregular. Lungs had decreased breath sounds. Abdomen was unremarkable.
Laboratory
His admission laboratory is unremarkable and include a creatinine of 1.0 mg/dL, blood urea nitrogen (BUN) of 18 mg/dL, white blood count (WBC) of 7.3 X 109 cells/L, and electrolytes with normal limits.
Radiography
His portable chest x-ray is shown in Figure 1.

Figure 1. Portable chest x-ray taken on admission to the ICU.
What should be done next? (Click on the correct answer to proceed to the second of five panels)
- Bedside echocardiogram
- Diuresis with a furosemide drip because of his weight gain and cardiomegaly
- Observation
- 1 and 3
- All of the above
Cite as: Loftsgard T, Hammill J. March 2016 critical care case of the month. Southwest J Pulm Crit Care. 2016;12(3):81-8. doi: http://dx.doi.org/10.13175/swjpcc018-16 PDF
Ultrasound for Critical Care Physicians: 50 Ways to Line Your Liver
Seth Skiles ACNP
Theresa Heynekamp MD MPH
Division of Pulmonary, Critical care and Sleep Medicine,
University of New Mexico School of Medicine
Albuquerque, NM USA
A 54-year-old man with a past medical history significant for traumatic brain injury and aspiration pneumonia presented with hypoxic respiratory failure secondary to foreign body aspiration.
On presentation, the patient was found to be hypoxic and tachypneic, requiring endotracheal intubation and mechanical ventilation. Bronchoscopy was performed with removal of extensive food particles throughout both lungs. The patient subsequently developed sepsis secondary to aspiration pneumonia. He became hypotensive, requiring central venous catheter placement for vasopressor therapy. A right subclavian central line was attempted under ultrasound guidance. A beside ultrasound was subsequently performed (Video 1).

What does the video obtained of a longitudinal view of the IVC at the level of the liver demonstrate? (Click on the correct answer for a discussion)
Cite as: Skiles S, Heynekamp T. Ultrasound for critical care physicians: 50 ways to line your liver. Southwest J Pulm Crit Care. 2015;11(5):235-7. doi: http://dx.doi.org/10.13175/swjpcc144-15 PDF
Ultrasound for Critical Care Physicians: The Martian
Jawad Abukhalaf, MD
Michel Boivin, MD
Division of Pulmonary, Critical care and Sleep Medicine,
University of New Mexico School of Medicine
Albuquerque, NM USA
A 54 year old male with a past medical history significant for granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis) and chronic kidney disease presented with hemoptysis and chest pain.
On presentation, he was found to have a 10 cm right middle lobe cavitary lesion and was subsequently treated with high dose steroids, antibiotics and antifungals based on bronchoalveolar lavage results. On day 9 of his hospital stay the patient was found to have bilateral lower extremity deep venous thromboses that were treated with intravenous heparin. On day 11 of his stay, the patient started experiencing lower abdominal pain and hypotension. The patient was resuscitated with saline. Bedside ultrasonography was performed.

Figure 1. Transverse lower abdominal ultrasound in the pelvis.
What does the transverse view of the lower abdomen (just above the symphysis pubis) demonstrate? (Click on the correct answer for an explanation)
Cite as: Abukhalaf J, Boivin M. Ultrasound for critical care physicians: the martian. Southwest J Pulm Crit Care. 2015;11(4):186-8. doi: http://dx.doi.org/10.13175/swjpcc135-15 PDF
March 2015 Critical Care Case of the Month: It’s Not Always Sepsis
Dionne Morgan, MD
Carolyn H. Welsh, MD
University of Colorado and the Eastern Colorado Veterans Affairs Medical Center
Department of Medicine
Division of Pulmonary Sciences and Critical Care Medicine
Denver, CO
History of Present Illness
A 57-year-old man with multiple co-morbidities including diabetes mellitus presented with wet gangrene of the right foot and hypotension. He had diabetic ketoacidosis and acute kidney injury. He was admitted to the medical intensive care unit, given intravenous fluids and treated with insulin therapy, piperacillin/tazobactam and vancomycin. Initial blood cultures grew Methicillin-resistant Staphylococcus aureus (MRSA). The podiatry service performed a right transmetatarsal amputation. Subsequently, he did well and was transferred to a medical floor for further care.
Three weeks later, following resolution of the initial sepsis, he developed persistently high fevers with hemodynamic instability despite continued antibiotic therapy. He was transferred back to the MICU for presumed sepsis.
Past Medical History, Social History and Family History
The past medical history was significant for diabetes, hypertension, COPD, coronary artery disease and hepatitis C. He did not smoke nor drink alcohol. Family history was non-contributory.
Physical Examination
On readmission to the medical intensive care unit, the patient was noted to have a generalized maculopapular rash on both upper and lower extremities, torso, palms and soles of his feet, associated with facial and periorbital edema (Figure 1). There was no mucosal membrane involvement or lymphadenopathy. He was also febrile to 104o F, hypotensive to 80/50 mm Hg and icteric.

Figure 1. Image of rash.
Laboratory Studies
Initial labs showed elevated leukocyte count, BUN and creatinine with anion-gap metabolic acidosis but a normal liver enzyme profile. Repeat labs on readmission to the medical ICU were significant for severe leukocytosis, with marked eosinophilia, atypical lymphocytes on blood smear, acute transaminitis and hyperbilirubinemia.
Admission labs: White blood cell count (WBC) 29.9 x 1000 cells/μL. Eosinophils 0.0% (Normal 0.0 - 0.7%), AST 28 U/L, ALT 15 U/L, ALP 162 U/L, total bilirubin 0.2 mg/dL.
Labs on ICU readmission: White blood cell count (WBC) 35.7 x 1000 cells/ μL. Eosinophils 2.3% (Normal 0.0 -0.7%), AST 486 U/L, ALT 288 U/L, ALP 749 U/L, total bilirubin 4.3 mg/dL.
Which are components of the SIRS criteria? (click on the correct answer to proceed to the second of 4 panels)
Reference as: Morgan D, Welsh CH. March 2015 critical care case of the month: it's not always sepsis. Southwest J Pulm Crit Care. 2015;10(3):105-11. doi: http://dx.doi.org/10.13175/swjpcc029-15 PDF
Analysis of a Fatal Left Ventricular Assist Device Infection: A Case Report and Discussion
Neal Stuart Gerstein, MD FASE1
Henry G. Chou, MD2
Andrew Lewis Dixon, MD1
1Department of Anesthesiology & Critical Care Medicine
University of New Mexico
Albuquerque, NM
2Department of Anesthesiology
Cedars-Sinai Medical Center
Los Angeles, CA
Introduction
Left ventricular assist device (VAD) therapy is an increasingly utilized treatment as a bridge to heart transplantation or as long-term destination therapy. Recent reports show there is a 22% - 32% incidence of VAD-associated infections with staphylococci and nosocomial gram-negative bacilli being the most common causative organisms (1,2). These organisms are often found in intensive care units, where they have the highest proportion of resistance, thus exposing already critically ill patients to the possibility of resistant organism VAD-associated infections (3). Mortality rates exceed 60% when sepsis develops in a patient with a continuous flow left VAD and infection is the number one cause of death in those awaiting cardiac transplantation (4,5). With continued left VAD use clinicians will likely see multidrug-resistant (MDR) or even pandrug-resistant organism VAD-associated infections. Clinicians need to be prepared to manage such an intimidating entity.
Case Report
We report a case of a 25 year-old male with a pandrug-resistant Pseudomonas aeruginosa VAD-associated infection. The patient’s medical history is significant for a diagnosis of idiopathic dilated cardiomyopathy refractory to maximal medical therapy requiring implantation of a HeartMate II (Thoratec Co., Pleasanton, CA, USA) continuous flow left VAD (Figure 1).

Figure 1. HeartMate II® left VAD schematic (reprinted with the permission of Thoratec Co., Pleasanton, CA, USA).
His course was complicated with multiple hospital admissions for recurrent VAD-associated infections and numerous episodes of P. aeruginosa bacteremia that had been treated with a multitude of antipseudomonal antibiotics. He presented to our hospital for management of severe volume overload in the setting of VAD-associated infections. Transesophageal echocardiography demonstrated a left ventricular ejection fraction of 24% with severe left and right ventricular dilatation. Chest x-ray revealed cardiomegaly and multiple devices including the left VAD (Figure 2).

Figure 2. Chest X-ray demonstrating an enlarged cardiac silhouette, the HeartMate II axial pump (*) with inflow (down arrow, ↓) and outflow (up arrow, ↑) cannulas, biventricular pacer with leads in right atrium (A), coronary sinus (B), and right ventricle (C) (dashed arrows).
Blood cultures revealed MDR P. aeruginosa; except for showing intermediate sensitivity to tobramycin there was resistance to all antimicrobials tested. In vitro synergy testing revealed modest bacterial inhibition when only colistin, fosfomycin, imipenem, and tobramycin were combined. After maximizing medical therapy, multiple left VAD pocket washings and implantation of tobramycin beads followed. Intraoperative findings included an encapsulated infection around the driveline and obvious infection of the left VAD pocket. Repeat blood cultures showed P. aeruginosa had developed resistance to all antimicrobials including tobramycin. Subsequently the left VAD was explanted and the patient was transitioned to an extracorporeal membrane oxygenator (ECMO) in attempt to clear the infection. He was then transitioned to a TandemHeart (CardiacAssist Inc., Pittsburgh, PA, USA), a percutaneous LVAD, as he was not dependent on ECMO for oxygenation. He was able to clear the bacteremia after removal of the infected HeartMate II while on colistin, fosfomycin, tobramycin, azithromycin and rifampin, but was not able to clear the remaining left VAD pocket infection, which again spread systemically. Despite maximal medical and surgical interventions, he died from profound septic shock and multisystem organ failure. To date this is the first known case of a pandrug-resistant P. aeruginosa VAD-associated infection reported in the literature.
Discussion
P. aeruginosa organisms have intrinsic resistance to numerous broad spectrum antibiotics, and can easily develop acquired resistance to most if not all available antimicrobial agents (3). Risk factors for the development of pandrug-resistant P. aeruginosa include previous treatment with antipseudomonal antibiotics and prolonged treatment times. Given our patient had multiple P. aeruginosa infections, treated with multiple rounds of antipseudomonal antibiotics, it is not surprising that pandrug-resistance developed. Few therapeutic options are available for treatment and no new agents are available to evade the known resistance mechanisms. Treatment can be optimized using synergistic combination therapy, which may be the only medical management option in patients with pandrug-resistant P. aeruginosa infections. Some have suggested that rifampin in combination with colistin may be a promising approach (3). Some experts recommend in vitro synergy testing when an organism is resistant to currently recommended antibiotic regimens (6,7). However, a recent review of antibiotic therapy for gram-negative infections describes the utility of in vitro synergy testing equivocal in the context of Pseudomonas infection (8). We managed our patient with combination therapy; however, not until pandrug-resistant P. aeruginosa was isolated did we introduce rifampin in combination with colistin.
A recent review of VAD-associated infections showed the majority were managed without surgical intervention; only 13% required surgical debridement and only in cases of severe infection and/or failed conservative treatment was left VAD explantation required. Since this case there has been a proposed algorithm for management of VAD-associated infections (2); our management, though prior to published guidelines, was in step with the algorithm. Of note, there was no discussion of explanting an left VAD to ECMO to aid in clearing a resistant infection. We felt this was a rational option given our inability to clear the infection. It is unclear as to exactly why our patient was never able to fully clear his infection. Given the patient’s other pre-existing extensive cardiac hardware (i.e. implanted pacer), it is possible that he remained colonized even after maximal surgical and medical therapy. Though speculative, it is possible that removing all foreign material may have allowed for complete infection clearance.
Aside from aggressive medical and surgical management, systolic heart failure with VAD-associated infections may be effectively managed with heart transplantation (9). Our consensus was that this option was neither in the best interest of the patient nor the best use of available resources given the severity of his condition.
Conclusion
Clinicians will continue to see VAD-associated infections with resistant organisms. To minimize adverse outcomes, including VAD-associated infection, prudent patient selection and timing of VAD placement is paramount, as VAD’s placed in critically ill patients have been consistently associated with adverse outcomes (10).
References
- Gordon RJ, Weinberg AD, Pagani FD, Slaughter MS, Pappas PS, Naka Y, Goldstein DJ, Dembitsky WP, Giacalone JC, Ferrante J, Ascheim DD, Moskowitz AJ, Rose EA, Gelijns AC, Lowy FD. Prospective, multicenter study of ventricular assist device infections. Circulation. 2013;127:691-702. [CrossRef] [PubMed]
- Nienaber JJ, Kusne S, Riaz T, Walker RC, Baddour LM, Wright AJ, Park SJ, Vikram HR, Keating MR, Arabia FA, Lahr BD, Sohail MR. Clinical manifestations and management of left ventricular assist device-associated infections. Clin Infect Dis. 2013;57:1438-48. [CrossRef] [PubMed]
- Zavascki AP, Carvalhaes CG, Picao RC, Gales AC. Multidrug-resistant Pseudomonas aeruginosa and Acinetobacter baumannii: resistance mechanisms and implications for therapy. Expert Rev Anti Infect Ther. 2010;8:71-93. [CrossRef] [PubMed]
- Topkara VK, Kondareddy S, Malik F, Wang IW, Mann DL, Ewald GA, Moazami N. Infectious complications in patients with left ventricular assist device: etiology and outcomes in the continuous-flow era. Ann Thorac Surg. 2010;90:1270-7. [CrossRef] [PubMed]
- Bartoli CR, Demarest CT, Khalpey Z, Takayama H, Naka Y. Current management of left ventricular assist device erosion. J Card Surg. 2013;28:776-82. [CrossRef] [PubMed]
- Balaji V, Jeremiah SS, Baliga PR. Polymyxins: Antimicrobial susceptibility concerns and therapeutic options. Indian J Med Microbiol. 2011;29:230-42. [CrossRef] [PubMed]
- Martis N, Leroy S, Blanc V. Colistin in multi-drug resistant Pseudomonas aeruginosa blood-stream infections: a narrative review for the clinician. J Infect. 2014;69:1-12. [CrossRef] [PubMed]
- Tamma PD, Cosgrove SE, Maragakis LL. Combination therapy for treatment of infections with gram-negative bacteria. Clin Microbiol Rev. 2012;25:450-70. [CrossRef] [PubMed]
- Prendergast TW, Todd BA, Beyer AJ, 3rd, Furukawa S, Eisen HJ, Addonizio VP, Browne BJ, Jeevanandam V. Management of left ventricular assist device infection with heart transplantation. Ann Thorac Surg. 1997;64:142-7. [CrossRef] [PubMed]
- Lietz K, Long JW, Kfoury AG, Slaughter MS, Silver MA, Milano CA, Rogers JG, Naka Y, Mancini D, Miller LW. Outcomes of left ventricular assist device implantation as destination therapy in the post-REMATCH era: implications for patient selection. Circulation. 2007;116:497-505. [CrossRef] [PubMed]
Reference as: Gerstein NS, Chou HG, Dixon AL. Analysis of a fatal left ventricular assist device infection: a case report and discussion. Southwest J Pulm Crit Care. 2015;10:16-20. doi: http://dx.doi.org/10.13175/swjpcc139-14 PDF
Ultrasound for Critical Care Physicians: Lung Sliding and the Seashore Sign
Spencer M. Lee, MD
Gregory T. Chu, MD
Banner Good Samaritan Medical Center
Phoenix, AZ
A 70-year-old Native American woman was having increasing difficulty with ventilation. She had an extensive past medical history including quadriplegia after a motor vehicle accident in 2009, chronic mechanical ventilation since the accident, end-stage renal disease, and diabetes mellitus. A feeding tube had recently been inserted. A portable chest radiograph was performed (Figure 1).

Figure 1. Portable chest radiograph.
A lung ultrasound was performed (Figure 2).


Figure 2. Lung ultrasound of the left lung (upper panel) and of the right lung (lower panel).
M-mode images of the ultrasound are shown in Figure 3.

Figure 3. M-mode image of the left lung (panel A on left) and the right lung (Panel B on right).
Which of the following are true regarding the images presented? (Click on the correct answer to procced to the next and final panel)
- The chest x-ray shows the feeding tube in the right lung
- The M-mode image shows the seashore sign on the left suggestive of a pneumothorax
- The ultrasound shows an absence of lung sliding on the right suggestive of a pneumothorax
- 1 and 3
- All of the above
Reference as: Lee SM, Chu GT. Ultrasound for critical care physicians: lung sliding and the seashore sign. Southwest J Pulm Crit Care. 2014;9(6):337-40. doi: http://dx.doi.org/10.13175/swjpcc163-14 PDF