
Critical Care
The Southwest Journal of Pulmonary and Critical Care publishes articles directed to those who treat patients in the ICU, CCU and SICU including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.

Delineating Gastrointestinal Dysfunction Variants in Severe Burn Injury Cases: A Retrospective Case Series with Literature Review
Sriharsha Rapaka MD 1,2
Priyankar Kumar Datta MD, DNB, DM 3
Shashikant Sharma MD, DM 3,4
1Intensive Care Medicine, St John of God Healthcare, Victoria, Australia
2Critical Care Medicine, All India Institute of Medical Sciences, New Delhi, India
3Anaesthesiology, Pain Medicine and Critical Care, All India Institute of Medical Sciences, New Delhi, India
4Critical Care Medicine, Jayaprabha Medanta Hospital, Patna, India
Abstract
Background: Severe burns can significantly impact various organ systems, including the gastrointestinal (GI) system. GI complications are frequently observed in patients with over 20% total body surface area (TBSA) burn.
Objectives: This case series delves into the intricate phenomenology of post-burn GI dysfunction, challenging conventional cause-and-effect paradigms. Our aim is to discern, comprehend, and explore variables influencing positive and negative outcomes, laying the foundation for further research given the current heterogeneity in the literature.
Methods: Severe burn patients with GI dysfunction identified between April 1, 2022, and July 31, 2022, from the institutional database are included in this retrospective case-series, and comparisons were made across baseline and treatment conditions across participants. Data were collected on demographics, burn characteristics, complications, and treatment outcomes.
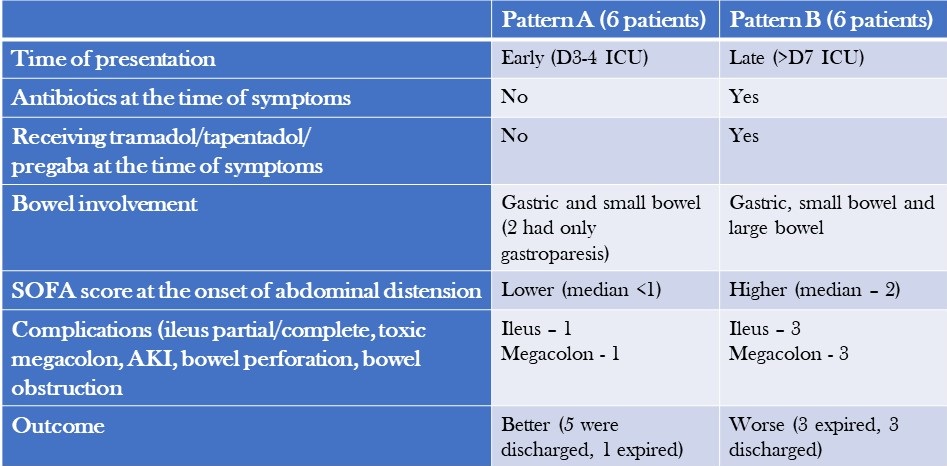
Results: We analysed 12 patients with severe burns and GI dysfunction and categorized them into two patterns: Pattern A, characterised by early onset symptoms, gastric and small bowel dilatation, and a relatively benign course with high recovery rates was observed in 6 patients; and Pattern B, characterised by late-onset symptoms, colonic dilatation, shock, and a high mortality rate due to megacolon was seen in 6 patients.
Conclusion: The post-burn GI dysfunction observed in our study is a complex interplay of multiple factors. Adequate fluid resuscitation, timely excision of necrotic tissue, staged food ingestion, specific nutrient administration, and appropriate use of antibiotics and judicious use of selective digestive decontamination (SDD) are essential strategies to prevent and treat this syndrome.
Introduction
Severe burns can have significant physiological impacts on the body, posing a risk to a patient's life that may be exacerbated by complications throughout the stages of treatment (1,2). Gastrointestinal (GI) complications are common in partial and full-thickness burns involving more than 20% TBSA and can include constipation, delayed gastric emptying, bacterial translocation, and sepsis, among others (2,3). While animal models suggest that burns delay gastric emptying and affect gut motility, the exact mechanism in humans is unknown (4,5). Probable causes could include large-volume fluid resuscitation, immobility, increased sympathetic drive secondary to pain, and dietary association with glutamine, opioids, and drugs such as tramadol and tapentadol. This study aims to describe two distinct patterns of bowel dysfunction observed in patients admitted with severe burns and discuss the impact of thermal injuries on gut motility and associated outcomes.
Methodology
Our study includes adult and paediatric patients with severe burns (>20% TBSA) and post-burn GI dysfunction, identified between April 1, 2022, and July 31, 2022. Data collection from discharge codes and chart reviews was conducted independently by two qualified, trained personnel for every participant from the medical records of eligible patients, employing anonymization protocols to uphold patient confidentiality during the entirety of the process. Data, including demographics, burn characteristics, complications, and response to treatment, were collected for the entire course of clinical care and subsequently compiled and reported. The burn unit at the hospital is staffed with highly skilled clinical staff members who have specialized training in treating severe burns. The assessment of treatments and data was supervised by an expert analyst at the faculty level.
Case Descriptions
The long-term outcome of a burn injury dramatically depends on the quality of care received during the initial hours. However, the majority of initial burn care is administered outside of specialized burn centres. It is essential to comprehend the intricacies of Advanced Burn Life Support (ABLS) to ensure the patient's optimal outcome. The medical team provided comprehensive intensive care to manage the patients' GI dysfunction and a description of the management, and treatment approach is summarised below.
- Symptoms: Patients with severe burns presented with symptoms such as diarrhoea, constipation, feed intolerance, abdominal distension, and hypoactive or diminished bowel sounds.
- Workup for diarrhoea: Patients underwent a workup that included testing for C. difficile toxin and stool culture and sensitivity, which both came back negative.
- Treatment for diarrhoea: Patients were treated with oral rehydration solution (ORS), probiotics, and racecadotril capsule (1.5mg/kg). Osmotic diarrhoea mostly resolved with reducing feed volume and protein content. In non-responders with suspected C. difficile infection presenting with fever, leucocytosis and pain abdomen, stool sample for toxin detection or culture was sent and oral metronidazole and, or oral vancomycin therapy was initiated. In patients who progressed to paralytic ileus, IV metronidazole along with oral vancomycin and vancomycin enema were administered.
- Treatment for constipation: Patients received syrup lactulose or syrup sodium picosulfate, liquid paraffin and milk of magnesia. Additionally, prokinetic agents were administered, and if necessary, enemas were used.
- Management of abdominal distension: In cases of abdominal distension, bowel decompression was performed by inserting a nasogastric tube with an intermittent suction system. This procedure aimed to reduce or resolve gastric dilatation, prevent vomiting and decrease the risk of aspiration associated with paralytic ileus.
- Intra-abdominal pressure (IAP) monitoring: Patients with abdominal distension underwent regular IAP monitoring, typically every 4 hours using indirect measurement via the bladder. If IAP exceeded 12 mmHg and was accompanied by hypotension, decreased urine output, or a tense abdomen, more frequent measurements (every 2 hours) were performed. Foley's catheter was also checked for blockage in case of increased IAP values. Monitoring continued until IAP levels dropped below 10 mmHg for several hours, along with clinical improvement.
- Stress ulcer prophylaxis and thromboprophylaxis: Patients above the age of 3 received pantoprazole for stress ulcer prophylaxis. Additionally, adult patients received injection Enoxaparin (1mg/kg) for thromboprophylaxis and mechanical prophylaxis. These measures were continued until patients achieved full ambulation.
- Antibiotics: Antibiotics were initiated only when signs of infection were observed, based on clinical assessment and monitoring of laboratory trends. Once definitive evidence of microbial growth from blood, urine, and wound cultures was obtained, culture-based antibiotics were started.
- Source control: Whenever necessary, the surgical team performed source control procedures to address and manage the underlying cause.
Patient Characteristics
Patients were separated into two patterns based on their clinical characteristics and outcomes (Table 1) and abdominal X-rays (Table 2).
Table 1. Comparison of the Two Patterns of Presentation (to view Table 1 in a new and separate window click here)
{kind=link}

- AKI=acute kidney injury
Table 2. Abdominal X-ray Patterns (to view Table 2 in a new and separate window click here)
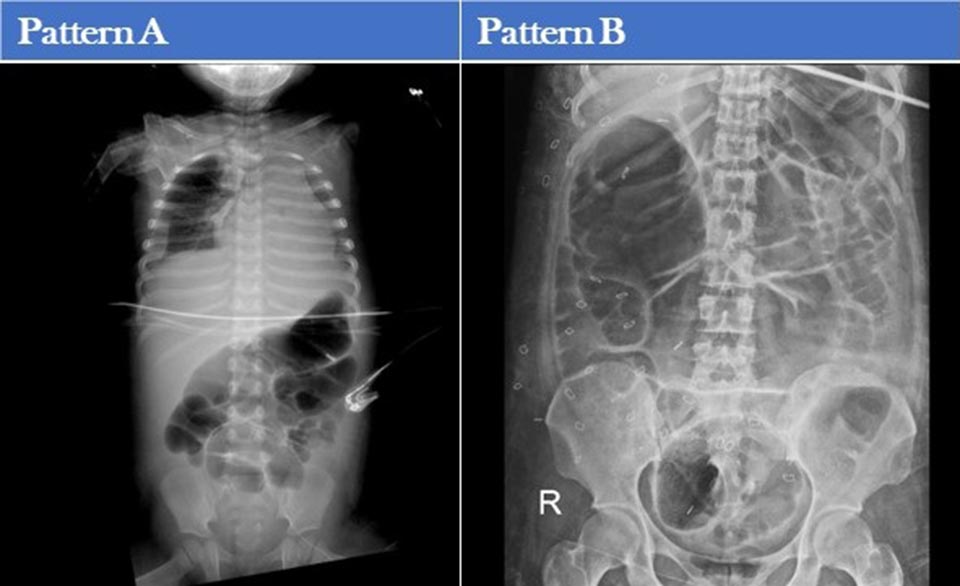{kind=link}

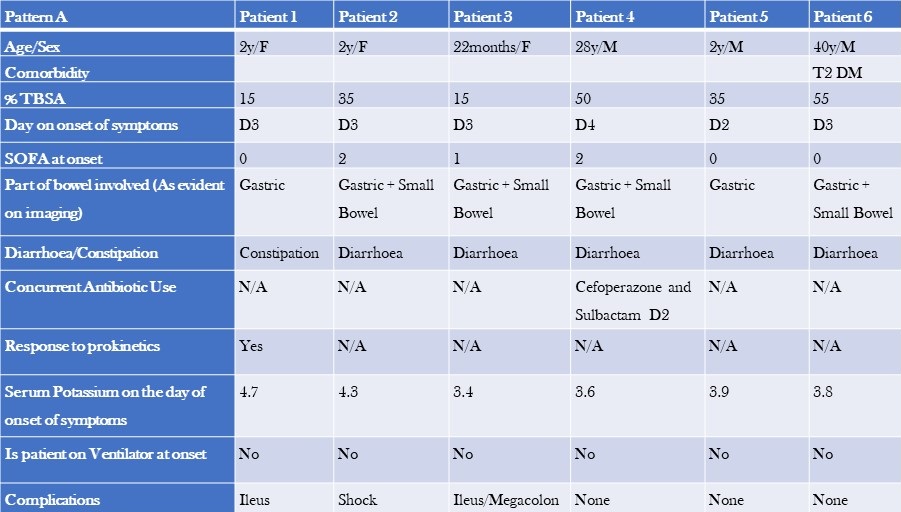
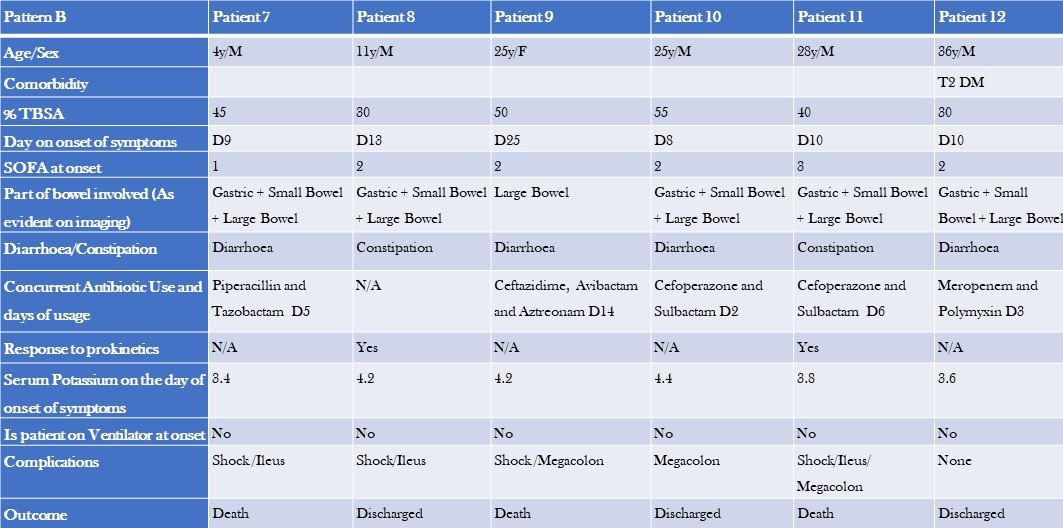
Additional patient characteristics of pattern A and B are shown tables 3 and 4.
Table 3. Clinical Characteristics, Laboratory, and Imaging Findings of Patients with Pattern A GI Dysfunction (to view Table 3 in a new and separate window click here)
{kind=link}

- TBSA=total burn surface area
- SOFA=Sequential Organ Failure Assessment Score
Table 4. Clinical Characteristics, Laboratory, and Imaging Findings of Patients with Pattern B GI Dysfunction (to view Table 4 in a new and separate window click here)
{kind=link}

The two groups differed in baseline characteristics. The first group had a smaller median TBSA compared to the second group (32.5% vs 42.5%). Additionally, the first group comprised primarily paediatric patients, and their GI dysfunction developed earlier (median day 3 vs day 10), with a lower median SOFA score (0 vs 1). The second group had colonic dilatation in addition to gastric and small bowel dilatation, and all patients had signs and, or evidence of infection and were on antibiotics by the time they developed GI dysfunction. The median serum potassium levels were also slightly different between the two groups (3.8 vs 4.2). Notably, there were more deaths in the second group (50%) compared to the first group, where most patients recovered and were shifted to a step-down unit.
Discussion
The stress response, metabolic changes, and nutritional deficiencies primarily cause most gastrointestinal (GI) issues associated with burn injuries. If not promptly recognized and appropriately treated, these complications can lead to severe consequences, including fatal haemorrhage or perforation. Implementing early prophylactic measures during the post-burn period is crucial to prevent these outcomes. One common complication of thermal injuries is gastric distention and dysfunction.
Studies have shown that gastric emptying is significantly reduced by approximately 37-42% at 6 hours after a burn (4-6). In our study, we observed early gastric dilation upon admission. Burn injuries also affect the standard slow wave frequency in the stomach, increasing the occurrence of bradygastria (7). However, patients who arrived at the emergency department within 2 hours of the burn injury and received timely resuscitation mostly remained asymptomatic. Radiological evidence revealed gastric dilation, which eventually resolved during their hospital stay.
Animal studies have demonstrated that small intestinal transit time is significantly decreased in burn injury models compared to control groups at 2 hours (8,9) and 6 hours post-burn (5,6,9,10). In our study, we observed early small bowel dilation and ileus during the ICU stay. Chen et al conducted a study with rat models, revealing that the gastrointestinal motility in burn-injured rats treated with saline is notably higher compared to untreated burn-injured rats (11). This finding aligns with our observations, as most patients who arrived early and received timely resuscitation showed resolution of bowel dilation.
Colonic transit time was delayed compared to the control group in burn injury patients (5,12). We could not find any literature on this topic in human subjects, highlighting the need for prospective studies. We noticed colonic involvement in symptomatic patients approximately one week after the burn injury. In cases of severe abdominal distension, dilated bowel loops, and feed intolerance, supplemental parenteral nutrition/TPN was administered. Early fluid resuscitation within 2 hours of a thermal injury is crucial in preventing multiple organ failure and mortality (18).
As described above, "Pattern A" patients experienced early symptoms during their ICU stay, showed minimal signs of infection, and had a relatively milder course with a lower mortality rate compared to "Pattern B" patients. Pattern B patients presented later, experienced more complications, and had higher morbidity and mortality rates. Dysmotility in these patients could be attributed to sepsis, opioids, or antibiotics. We tested for C. difficile toxin and culture, which came back negative. Immobility, opioid use, pain, and dietary glutamine are common causes of GI dysfunction in both patient groups. Incremental fentanyl infusion was administered to all patients within 24-48 hours of the injury. Breakthrough and procedural pain were managed with sub-anaesthetic doses of IV ketamine and IV fentanyl. Patients presenting with Pattern B symptoms were often prescribed slow-release oral tramadol/oral tapentadol/ pregabalin formulations to supplement or replace opioids due to concerns about constipation, tolerance, and addiction. Opioids could exacerbate GI symptoms like vomiting and constipation (14). Tramadol was found to delay colonic transit but did not affect upper gastrointestinal transit.15 Tapentadol, on the other hand, provided analgesia with a more tolerable side effect profile and resulted in less deterioration of gastrointestinal function and symptoms compared to standard opioids (16,17). However, results from different studies on tapentadol’ s effects on gastric emptying and bowel function are inconsistent, making its routine use in severe burns unclear (18,19). NSAIDs are effective for mild to moderate burns, but opioids are preferred in severe cases due to acute kidney injury (AKI) concerns. AKI is common in severe burns and an independent mortality risk factor. While opioids and NSAIDs may have contributed to large bowel dysmotility in Pattern B patients, a causal relationship cannot be established.
Burn-injured patients often experience acute and chronic neuropathic pain. Pregabalin has shown efficacy in reducing neuropathic pain and improving sleep but may cause constipation (20,21). Stress ulcer prophylaxis with pantoprazole was administered to patients above three years of age. Short-term treatment with proton pump inhibitors (PPIs) has been reported to delay gastric emptying of solid meals in healthy individuals (22). The effects of PPIs on liquid emptying are inconsistent (23). Prolonged gastric residence of PPIs due to delayed emptying may impact their pharmacological effectiveness, which can be clinically relevant in managing conditions such as GERD, functional dyspepsia, and diabetes (24). However, routine administration of PPIs in severe burn patients is not recommended. Although a systematic review and meta-analysis suggested a potential correlation between the usage of proton pump inhibitors (PPIs) and a heightened likelihood of contracting Clostridium difficile infection (CDI), we did not find any substantiating evidence of CDI (25). Further high-quality and prospective studies are needed to establish a causal relationship.
Major burns trigger an inflammatory response and catabolism, which can lead to severe nutrition deficiencies when combined with burn wound nutrient losses. These deficiencies can impair immune function and wound healing and increase the risk of organ injury and mortality (26). Sepsis causes dysbiosis and bacterial translocation (27). Severe burn patients frequently experience sepsis-induced ileus (28). Early and staged enteral nutrition has been shown to reduce gram-negative bacteraemia in burn patients and promote a healthy intestinal microenvironment (29-32). Caloric requirements were calculated using the Curreri formula for adults and Curreri junior formula for paediatric patients. However, as the formula often overestimates caloric needs, a target of 70-80% of the calculated requirement was set. Using continuous feeding bags, oral and/or nasogastric feeding was initiated from day 1 in the ICU. Post-pyloric feeding was administered to patients with feed intolerance or high gastric residual volume. Micronutrients and trace elements were supplemented, and glutamine and fibre were added to the diet for adult patients. Glutamine stimulates the release of glucagon-like peptide-1, which increases postprandial insulin secretion and slows gastric emptying (33). Current recommendations support using glutamine in severe burn patients due to promising evidence and minimal adverse effects. The RE-ENERGIZE trial showed mortality at 6 months was 17.2% in the glutamine group and 16.2% in the placebo group (hazard ratio for death, 1.06; 95% CI, 0.80 to 1.41) and no substantial between-group differences in serious adverse events (26).
We hypothesize that prudent utilization of selective digestive decontamination (SDD) may reduce infections and improve survival in severe burn patients (34). In a randomized trial, SDD demonstrated improved survival. However, according to a meta-analysis, enteral antibiotic use did not reduce mortality in severe burn patients, which aligns with our findings (35).
Managing wounds in the early stages and providing postoperative care after skin grafting pose challenges in patients with extensive burns. Effective use of negative pressure wound therapy (NPWT) can facilitate better wound healing and reduce infections. Patients with burns involving the perineum and genitalia present particular challenges due to increased wound infections, graft loss, and sepsis caused by dressing soiling (36-38). We hypothesize that faecal management systems might reduce infections by diverting faeces and improving personal hygiene in severe burn patients. A retrospective study found a survival benefit with no significant complications associated with faecal management systems (39).
Limitations
Our study is a retrospective case series that has inherent constraints. Our study lacked a control group. Selection bias and treatment assignment bias cannot be ruled out. These unregulated and unidentified factors of variation have the potential to influence the general applicability of the study's outcomes. Further prospective studies are needed to establish causal associations.
Conclusions
The first pattern of patients, primarily children without underlying health conditions, appeared to have experienced bowel dysfunction as a stress response amplified using PPIs. Diarrhoea in these cases was not due to an infection, and excessive sympathetic activity could be the contributing factor. On the other hand, the second pattern of patients, primarily adults with comorbidities, were seriously ill and received a combination of antibiotics, opioids, and gabapentin. These patients were also experiencing sepsis and sepsis-induced ileus, which is common in individuals with severe burns. In this group, diarrhoea could be caused by an infectious or non-infectious agent, and while testing for C. difficile was negative, there may have been delays in the transportation and analysis of stool samples that resulted in false negative results. It is important to note that repeating the tests is unlikely to improve the sensitivity of the results (40).Top of Form
Learning Points
- Post-burn gastrointestinal issues are caused by a combination of factors that disrupt the balance of gut microbes leading to sepsis and multiple organ dysfunction syndrome (MODS).
- Further prospective studies are needed to establish the effect of tramadol, tapentadol and pregabalin on GI system in severe burns.
- The regular use of PPIs may worsen the impact of severe burns on the gut.
- Managing serious burns necessitates a collaborative strategy encompassing prompt and effective fluid replacement, timely removal of deceased tissue, cautious initiation of nutrition, targeted use of antibiotics, and thoughtful application of selective digestive decontamination (SDD) to prevent gastrointestinal complications and reduce mortality.
- Faecal management systems and negative pressure wound therapy (NPWT) can help to improve wound care and hygiene in patients with perineal burns.
References
- Jeschke MG, Pinto R, Kraft R, Nathens AB, Finnerty CC, Gamelli RL, Gibran NS, Klein MB, Arnoldo BD, Tompkins RG, Herndon DN; Inflammation and the Host Response to Injury Collaborative Research Program. Morbidity and survival probability in burn patients in modern burn care. Crit Care Med. 2015 Apr;43(4):808-15. [CrossRef] [PubMed]
- Jonason AM. Complications of burn injury. Occup Health Nurs. 1983 Jul;31(7):24-8. [CrossRef] [PubMed]
- Czaja AJ, McAlhany JC, Pruitt BA Jr. Acute gastroduodenal disease after thermal injury. An endoscopic evaluation of incidence and natural history. N Engl J Med. 1974 Oct 31;291(18):925-9. [CrossRef] [PubMed]
- Sallam HS, Kramer GC, Chen JD. Gastric emptying and intestinal transit of various enteral feedings following severe burn injury. Dig Dis Sci. 2011 Nov;56(11):3172-8. [CrossRef] [PubMed]
- Sallam HS, Oliveira HM, Gan HT, Herndon DN, Chen JD. Ghrelin improves burn-induced delayed gastrointestinal transit in rats. Am J Physiol Regul Integr Comp Physiol. 2007 Jan;292(1):R253-7. [CrossRef] [PubMed]
- Oliveira HM, Sallam HS, Espana-Tenorio J, Chinkes D, Chung DH, Chen JD, Herndon DN. Gastric and small bowel ileus after severe burn in rats: the effect of cyclooxygenase-2 inhibitors. Burns. 2009 Dec;35(8):1180-4. [CrossRef] [PubMed]
- Sallam HS, Oliveira HM, Liu S, Chen JD. Mechanisms of burn-induced impairment in gastric slow waves and emptying in rats. Am J Physiol Regul Integr Comp Physiol. 2010 Jul;299(1):R298-305. [CrossRef] [PubMed]
- Alican I, Coşkun T, Yeğen C, Aktan AO, Yalin R, Yeğen BC. The effect of thermal injury on gastric emptying in rats. Burns. 1995 May;21(3):171-4. [CrossRef] [PubMed]
- Unlüer EE, Alican I, Yeğen C, Yeğen BC. The delays in intestinal motility and neutrophil infiltration following burn injury in rats involve endogenous endothelins. Burns. 2000 Jun;26(4):335-40. [CrossRef] [PubMed]
- Oktar BK, Cakir B, Mutlu N, Celikel C, Alican I. Protective role of cyclooxygenase (COX) inhibitors in burn-induced intestinal and liver damage. Burns. 2002 May;28(3):209-14. [CrossRef] [PubMed]
- Chen CF, Chapman BJ, Munday KA, Fang HS. The effects of thermal injury on gastrointestinal motor activity in the rat. Burns Incl Therm Inj. 1982 Nov;9(2):142-6. [CrossRef] [PubMed]
- Gan HT, Chen JD. Roles of nitric oxide and prostaglandins in pathogenesis of delayed colonic transit after burn injury in rats. Am J Physiol Regul Integr Comp Physiol. 2005 May;288(5):R1316-24. [CrossRef] [PubMed]
- Barrow RE, Jeschke MG, Herndon DN. Early fluid resuscitation improves outcomes in severely burned children. Resuscitation. 2000 Jul;45(2):91-6. [CrossRef] [PubMed]
- Melchior C, Desprez C, Wuestenberghs F, Leroi AM, Lemaire A, Goucerol G. Impact of Opioid Consumption in Patients With Functional Gastrointestinal Disorders. Front Pharmacol. 2020 Dec 21;11:596467. [CrossRef] [PubMed]
- Wilder-Smith CH, Bettiga A. The analgesic tramadol has minimal effect on gastrointestinal motor function. Br J Clin Pharmacol. 1997 Jan;43(1):71-5. [CrossRef] [PubMed]
- Singh DR, Nag K, Shetti AN, Krishnaveni N. Tapentadol hydrochloride: A novel analgesic. Saudi J Anaesth. 2013 Jul;7(3):322-6. [CrossRef] [PubMed]
- Etropolski M, Kelly K, Okamoto A, Rauschkolb C. Comparable efficacy and superior gastrointestinal tolerability (nausea, vomiting, constipation) of tapentadol compared with oxycodone hydrochloride. Adv Ther. 2011 May;28(5):401-17. [CrossRef] [PubMed]
- Mark EB, Nedergaard RB, Hansen TM, Nissen TD, Frøkjaer JB, Scott SM, Krogh K, Drewes AM. Tapentadol results in less deterioration of gastrointestinal function and symptoms than standard opioid therapy in healthy male volunteers. Neurogastroenterol Motil. 2021 Nov;33(11):e14131. [CrossRef] [PubMed]
- Jeong ID, Camilleri M, Shin A, et al. A randomised, placebo-controlled trial comparing the effects of tapentadol and oxycodone on gastrointestinal and colonic transit in healthy humans. Aliment Pharmacol Ther. 2012 May;35(9):1088-96. [CrossRef] [PubMed]
- Gray P, Kirby J, Smith MT, Cabot PJ, Williams B, Doecke J, Cramond T. Pregabalin in severe burn injury pain: a double-blind, randomised placebo-controlled trial. Pain. 2011 Jun;152(6):1279-1288. [CrossRef] [PubMed]
- Toth C. Pregabalin: latest safety evidence and clinical implications for the management of neuropathic pain. Ther Adv Drug Saf. 2014 Feb;5(1):38-56. [CrossRef] [PubMed]
- Kurt A, Altun A, Bağcivan I, Koyuncu A, Topcu O, Aydın C, Kaya T. Effects of proton pump inhibitors and h(2) receptor antagonists on the ileum motility. Gastroenterol Res Pract. 2011;2011:218342. [CrossRef] [PubMed]
- Sanaka M, Yamamoto T, Kuyama Y. Effects of proton pump inhibitors on gastric emptying: a systematic review. Dig Dis Sci. 2010 Sep;55(9):2431-40. [CrossRef] [PubMed]
- Baron JH. The pharmacology of gastric acid. Scand J Gastroenterol Suppl. 1983;18(87):7-23.
- Trifan A, Stanciu C, Girleanu I, Stoica OC, Singeap AM, Maxim R, Chiriac SA, Ciobica A, Boiculese L. Proton pump inhibitors therapy and risk of Clostridium difficile infection: Systematic review and meta-analysis. World J Gastroenterol. 2017 Sep 21;23(35):6500-6515. [CrossRef] [PubMed]
- Wischmeyer PE. Glutamine in Burn Injury. Nutr Clin Pract. 2019 Oct;34(5):681-687. [CrossRef] [PubMed]
- Fay KT, Ford ML, Coopersmith CM. The intestinal microenvironment in sepsis. Biochim Biophys Acta Mol Basis Dis. 2017 Oct;1863(10 Pt B):2574-2583. [CrossRef] [PubMed]
- Kirksey TD, Moncrief JA, Pruitt BA Jr, O'Neill JA Jr. Gastrointestinal complications in burns. Am J Surg. 1968 Nov;116(5):627-33. [CrossRef] [PubMed]
- Huang HH, Lee YC, Chen CY. Effects of burns on gut motor and mucosa functions. Neuropeptides. 2018 Dec;72:47-57. [CrossRef] [PubMed]
- He W, Wang Y, Wang P, Wang F. Intestinal barrier dysfunction in severe burn injury. Burns Trauma. 2019 Jul 26;7:24. [CrossRef] [PubMed]
- Earley ZM, Akhtar S, Green SJ, et al. Burn Injury Alters the Intestinal Microbiome and Increases Gut Permeability and Bacterial Translocation. PLoS One. 2015 Jul 8;10(7):e0129996. [CrossRef} [PubMed]
- Xiao SC, Zhu SH, Xia ZF, Lu W, Wang GQ, Ben DF, Wang GY, Cheng DS. Prevention and treatment of gastrointestinal dysfunction following severe burns: a summary of recent 30-year clinical experience. World J Gastroenterol. 2008 May 28;14(20):3231-5. [CrossRef] [PubMed]
- Du YT, Piscitelli D, Ahmad S, Trahair LG, Greenfield JR, Samocha-Bonet D, Rayner CK, Horowitz M, Jones KL. Effects of Glutamine on Gastric Emptying of Low- and High-Nutrient Drinks in Healthy Young Subjects-Impact on Glycaemia. Nutrients. 2018 Jun 7;10(6):739. [CrossRef] [PubMed]
- de La Cal MA, Cerdá E, García-Hierro P, van Saene HK, Gómez-Santos D, Negro E, Lorente JA. Survival benefit in critically ill burned patients receiving selective decontamination of the digestive tract: a randomized, placebo-controlled, double-blind trial. Ann Surg. 2005 Mar;241(3):424-30. [CrossRef] [PubMed]
- Rubio-Regidor M, Martín-Pellicer A, Silvestri L, van Saene HKF, Lorente JA, de la Cal MA. Digestive decontamination in burn patients: A systematic review of randomized clinical trials and observational studies. Burns. 2018 Feb;44(1):16-23. [CrossRef] [PubMed]
- Gómez-Ortega V, Vergara-Rodriguez MJ, Mendoza B, García T. Effect of Negative Pressure Wound Therapy in Electrical Burns. Plast Reconstr Surg Glob Open. 2021 Feb 17;9(2):e3383. [CrossRef] [PubMed]
- Teng SC. Use of negative pressure wound therapy in burn patients. Int Wound J. 2016 Sep;13 Suppl 3(Suppl 3):15-8. [CrossRef] [PubMed]
- Kantak NA, Mistry R, Varon DE, Halvorson EG. Negative Pressure Wound Therapy for Burns. Clin Plast Surg. 2017 Jul;44(3):671-677. [CrossRef] [PubMed]
- Farroha A, Frew Q, Philp B, Dziewulski P. Improvement of survival in patients with extensive burns involving the perineum with use of a faecal management system. Ann Burns Fire Disasters. 2014 Mar 31;27(1):14-6. [PubMed]
- Bagdasarian N, Rao K, Malani PN. Diagnosis and treatment of Clostridium difficile in adults: a systematic review. JAMA. 2015 Jan 27;313(4):398-408. [CrossRef] [PubMed]
Severe Accidental Hypothermia in Phoenix? Active Rewarming Using Thoracic Lavage
Michael Mozer BS1
Guy Raz, MD2
Ryan Wyatt, MD2
Alexander Toledo, DO, PharmD2
1University of New England College of Osteopathic Medicine
Biddeford, ME USA
2Department of Emergency Medicine
Maricopa Medical Center, Phoenix, AZ USA
Abstract
Hypothermia can progress quickly and become life threatening if left untreated. Rewarming in the severely hypothermic patient is of critical importance and is achieved with active and passive techniques. Here we present a case of a hypothermic patient with cardiac instability for whom thoracic lavage was ultimately used. We will review the treatment of hypothermia and discuss the technical aspects our approach.
Case Presentation
A 53 year-old male with a past medical history of substance abuse, chronic hepatitis C, and poorly controlled type 2 diabetes mellitus complicated by a recent hospitalization for osteomyelitis was brought to the emergency department after being found lying on a road in a shallow pool of water in the early morning hours of a rainy day in Phoenix, Arizona. The ambient temperature that night was 39 °F (3.9 °C). Emergency Medical Services (EMS) noted a decreased level of consciousness and obtained a finger stick glucose of 15 mg/dl. EMS reported a tympanic membrane temperature of 23.9 °C. En route, the patient was administered 2mg naloxone and 25g dextrose intravenously with no improvement in his mental status. On Emergency Department (ED) arrival, the patient had a GCS of 8 (Eyes 4, Verbal 1, Motor 3) and exhibited intermittent posturing. His foot wound appeared clean and without signs of infection. The initial core temperature recorded was 25.9°C via bladder thermometer, systolic blood pressure was 92/50, and heart rate fluctuated between 50 and 90 beats per minute.
After removing wet clothing, initiation of warmed saline, and placing a forced warm air blanket on the patient, he was intubated for airway protection and vasopressors were initiated. Osborn waves were evident on the initial EKG (Figure 1).

Figure 1. Initial EKG with Osborn Waves (arrows).
A warmed ventilator circuit was initiated with only 0.5 °C increase in temperature in first 30 minutes. Despite these measures, he remained hypotensive and unstable. Significant laboratory findings were a white blood cell count of 25.5 thousand (92% neutrophils), lactic acid of 7.6, potassium of 5.8, serum creatinine of 1.05, glucose of 283, INR of 1.1, and urine drug screen positive for cocaine. Given his recalcitrance to norepinephrine and risk of death secondary to fatal dysrhythmia with temperatures below 28 °C intrathoracic lavage initiated.
The right hemithorax was selected for irrigation because left-sided tube placement can induce ventricular fibrillation in a perfusing patient (1). Using standard sterile technique, two 36 French thoracostomy tubes were placed; the first in the second intercostal space along the mid-clavicular line, and the second in the 5th intercostal space in the posterior axillary line (1-3). The tips of the thoracostomy tubes were oriented such that the anterior-superior tube was positioned near the right apex and the lateral-inferior tip was positioned low in the thoracic cavity (1,3). To maintain the temperature of the instilled fluid, a fluid warmer system (Level 1; Smiths Medical; Minneapolis, MN) was used and set to 41 °C. A Christmas tree adapter was used to connect the IV tubing to the superior thoracostomy tube, and a water seal chamber was attached to the inferior tube for passive drainage (3). Flow through the system was targeted to maintain steady passive drainage as described in the literature (1-6).
Thoracic cavity lavage with 41 °C saline was performed and the patient was transferred to the medical ICU after 3 hours in the ED. When he was transferred his core temperature was 29 °C and he remained on norepinephrine for hemodynamic instability. After 2 hours of continued rewarming in the MICU, his core temperature was 32 °C. Osborn waves evident on initial EKG were resolved (Figure 2).

Figure 2. Repeat EKG showing resolution of Osborn waves.
The patient left against medical advice from the hospital 4 days later neurologically intact and without sequela.
Discussion
Hypothermia can be clinically classified as mild, moderate or severe (7). Mild hypothermia, defined as core temperatures of 32-35 °C, presents with shivering. Amnesia, dysarthria, ataxia, tachycardia, and tachypnea can also be seen (1). Moderate hypothermia, defined as core temperatures of 28-32 °C, usually can present with or without shivering. Stupor, hypoventilation, paradoxical undressing and non-fatal arrhythmias such as atrial fibrillation and junctional bradycardia may also be seen (1). Patients with severe hypothermia, generally defined as temperatures below 28 °C, can present with coma, areflexia, pulmonary edema, bradycardia, and hypotension (1). There is a significant risk of fatal cardiac dysrhythmias without rapid therapeutic rewarming (1,7,8).
Rewarming in the hypothermic patient is of critical importance and is achieved with passive and/or active techniques. Attempts to limit heat loss are often unsuccessful, especially in the absence of a normal shiver response. It however remains as the first line treatment for hypothermia (8-10). Passive rewarming is attempted by the removal of cold/wet clothing and keeping the patient covered (8-10). Active external rewarming (AER) is the next line of treatment and consist of the use of externally rewarming devices such as warmed blankets, warm environment, forced air warming (Bair Hugger; 3M; Maplewood, MN) or warm hot water bladders placed in the groin and axilla (1,7-10). Active Internal Rewarming (AIR) techniques can be used to achieve more rapid increases in core temperature and are primarily utilized in cases of cardiac instability or if AER is unsuccessful (8). When available, the method of choice for active internal rewarming (AIR) is cardiopulmonary bypass (CPB) or extracorporeal membrane oxygenation (ECMO) as they can achieve the fastest increase in core temperature (9 °C/hr and 6 °C/hr respectively) and provide cardiovascular support (1,8,11,12). Several techniques are described in the literature that can be considered if CPB or ECMO are unavailable. These include esophageal warming devices, endovascular catheters, hemodialysis, and endocavitary lavage (1,2,4-6,13-15). While no randomized controlled trials exist, several case reports and reviews have tried to compare various techniques. These sources to do not seem to favor any particular technique over another but rather reports the rates of temperature rise (1-3,5-7,13-15). Classically, lavage techniques are attempted in the thoracic cavity, the peritoneum, the bladder, the stomach, the esophagus, or the colon. These techniques are generally coupled with warm IV fluids and warming air through the ventilator to limit loss of body heat to iatrogenic procedures during the rewarming attempt (1,7). Thoracic lavage is effective with a reported rewarming rates of 3-6 °C/hr and with excellent outcomes in case reports (1,2,4-6). Here we present a case of a hypothermic patient with cardiac instability where thoracic lavage is used and discuss the technical aspects of this approach.
Our case demonstrates the efficacy of utilizing thoracic cavity lavage for rapid rewarming in patients with severe hypothermia with a pulse and at high risk of fatal cardiac arrhythmia. In multiple case reports, thoracic lavage has been used successfully in hypothermic patients who suffered complete cardiopulmonary collapse requiring CPR (2,4,5). Although warm thoracic lavage is not the treatment of choice in these circumstances, in a facility not equipped with ECMO or CPB and a patient too unstable to transfer, it seemed to us to be the best technique. Gastric, colonic, and bladder lavage offer very minimal heat transfer due to limitations in surface area (2).
Hemodialysis would have required for us to call in a technician and would have required approval by a nephrologist at our institution. Available central venous rewarming catheters require bypass of a failsafe mechanism that does not allow rewarming to be initiated below 30 °C (1). Peritoneal lavage was a plausible choice but does not directly warm the mediastinum (2). While an open mediastinal technique has been used, we did not feel it was appropriate in a patient with a concurrent pulse (1,3). Thoracic lavage is therefore an effective alternative that should be used in cases where CPB and ECMO are unavailable especially in a patient that is hemodynamically unstable and may not survive transfer. The equipment is readily available to any Emergency Medicine or Critical Care physician. In addition, this case exemplifies the positive outcomes that are associated with rapid rewarming in the hypothermic patient with a pulse. We believe our case demonstrates the efficacy of this technique for myocardial protection from hemodynamic collapse, a topic which has not been adequately studied in the literature.
References
- Brown DJ, Danzl DF. Accidental hypothermia. In: Auerbach PS, ed. Wilderness Medicine. 7th ed. St. Louis: Mosby Inc.; 2017:135-62.
- Plaisier BR. Thoracic lavage in accidental hypothermia with cardiac arrest--report of a case and review of the literature. Resuscitation. 2005 ;66(1):99-104. [CrossRef] [PubMed]
- Schiebout JD. Hypothermic Patient Management. In: Reichman EF. eds. Reichman's Emergency Medicine Procedures, 3e New York, NY: McGraw-Hill. Available at: http://accessemergencymedicine.mhmedical.com/content.aspx?bookid=2498§ionid=201303754 (accessed August 02, 2019).
- Little G. Accidental hypothermic cardiac arrest and rapid mediastinal warming with pleural lavage: A survivor after 3.5 hours of manual CPR. BMJ Case Reports. July 2017:bcr-2017-220900. [CrossRef] [PubMed]
- Turtiainen J, Halonen J, Syväoja S, Hakala T. Rewarming a patient with accidental hypothermia and cardiac arrest using thoracic lavage. Ann Thorac Surg. 2014 Jun;97(6):2165-6. [CrossRef] [PubMed]
- Ellis MM, Welch RD. Severe hypothermia and cardiac arrest successfully treated without external mechanical circulatory support. Am J Emerg Med. 2016;34(9):1913.e5-6. [CrossRef] [PubMed]
- Tintinalli J, Stapczynski J, Ma O, Yealy D, Meckler G, Cline D. Tintinalli's Emergency Medicine. 8th ed. New York, NY: McGraw-Hill Education; 2016:1743-4.
- Brugger H, Boyd J, Paal P. Accidental Hypothermia. N Engl J Med. 2012;367(20):1930-8. [CrossRef] [PubMed]
- Paal P, Gordon L, Strapazzon G, et al. Accidental hypothermia-an update: The content of this review is endorsed by the International Commission for Mountain Emergency Medicine (ICAR MEDCOM). Scand J Trauma Resusc Emerg Med. 2016;24(1):111. [CrossRef] [PubMed]
- Zafren K, Giesbrecht GG, Danzl DF, et al. Wilderness Medical Society practice guidelines for the out-of-hospital evaluation and treatment of accidental hypothermia: 2014 update. Wilderness Environ Med. 2014 Dec;25(4 Suppl):S66-85. [CrossRef] [PubMed]
- Schober A, Sterz F, Handler C, et al. Cardiac arrest due to accidental hypothermia-A 20 year review of a rare condition in an urban area. Resuscitation. 2014;85(6):749-56. [CrossRef] [PubMed]
- Saczkowski RS, Brown DJA, Abu-Laban RB, Fradet G, Schulze CJ, Kuzak ND. Prediction and risk stratification of survival in accidental hypothermia requiring extracorporeal life support: An individual patient data meta-analysis. Resuscitation. 2018;127:51-7.[CrossRef] [PubMed]
- Primozic KK, Svensek F, Markota A, Sinkovic A. Rewarming after severe accidental hypothermia using the esophageal heat transfer device: a case report. Ther Hypothermia Temp Manag. 2018 Mar;8(1):62-4. [CrossRef] [PubMed]
- Murakami T, Yoshida T, Kurokochi A, et al. Accidental hypothermia treated by hemodialysis in the acute phase: three case reports and a review of the literature. Intern Med. 2019 Jun 7. [CrossRef]
- Klein LR, Huelster J, Adil U, et al. Endovascular rewarming in the emergency department for moderate to severe accidental hypothermia. Am J Emerg Med. 2017 Nov;35(11):1624-9. [CrossRef] [PubMed]
Cite as: Mozer M, Raz G, Wyatt R, Toledo A. Severe accidental hypothermia in Phoenix? Active rewarming using thoracic lavage. Southwest J Pulm Crit Care. 2019;19(2):79-83. doi: https://doi.org/10.13175/swjpcc038-19 PDF
Carotid Cavernous Fistula: A Case Study and Review
Iaswarya Ganapathiraju, OMS-IV1
Douglas T Summerfield, MD2
Melissa M Summerfield, MD2
1Des Moines University College of Osteopathic Medicine
Des Moines, IA USA
2Mercy Medical Center North Iowa and North Iowa Eye Clinic
Mason City, IA USA
Abstract
Carotid cavernous fistulas are rare complications of craniofacial trauma, resulting in abnormal connections between the arterial and venous systems of the cranium. The diagnosis of carotid cavernous fistulas and other injuries as a result of trauma can be confounded by the traumatized patient’s inability to communicate their symptoms to their physician. The following case study demonstrates the importance of a thorough physical exam in caring for such patients and serves to remind physicians to have a low threshold for consultation when managing numerous injuries following trauma.
Introduction
Carotid cavernous fistulas (CCFs) are aberrant connections between the carotid arterial system and the cavernous sinus, which form as complications of craniofacial trauma, or are congenital or spontaneous in nature (1). They occur in up to 3.8% of patients with basilar skull fractures and are more common with middle fossa fracture (2). Prompt diagnosis and treatment of CCF is necessary as approximately 20 – 30% of carotid cavernous fistulas lead to vision loss if not addressed appropriately (3)/\The following is a case study of a patient who presented with multiple traumatic injuries including CCF with subsequent discussion of the typical presentation, diagnosis, and treatment of direct CCF.
Case Presentation
A 64-year-old woman with a therapeutic INR on Coumadin for atrial fibrillation sustained a fall down a flight of stairs. She was found unresponsive the next day by her relatives and was subsequently brought to the emergency department for evaluation. A maxillofacial CT showed a nondisplaced right maxillary wall fracture and nondisplaced zygomatic arch fracture, as well as a subtle inferotemporal orbital fracture, none of which was determined to require immediate treatment by the otolaryngology service. Further imaging included a CT of the head which revealed a large subdural hematoma, a superotemporal hematoma, and subfalcine herniation. She was taken to the OR for emergent craniotomy and evacuation of the hematoma before transfer to the critical care unit. In the CCU, she remained intubated and sedated but her condition improved until extubation on hospital day 3. She continued to have swelling surrounding both eyes during this time, but physical exam showed pupils which were equal, round, and reactive to light.
On day 6 of her stay, the patient was noted to have waxing and waning confusion and slightly increased oxygen requirement. Thus, she was re-intubated and sedated for “agitation” and “hypoxic respiratory failure.” Physical exam on the next day was notable for pupillary anisocoria with the right pupil at 1 mm diameter and left at 2.5 mm. There was a poor pupillary light reaction bilaterally. Neurology was consulted and recommended repeat imaging and EEG. Repeat CT and MRI of the brain showed no evidence of herniation, and EEG was negative for seizure-like activity. The anisocoria was thought to be from mass effect of the temporal lobe on cranial nerve III. The patient’s condition continued to deteriorate; physical exam elicited grimace to painful stimuli and the patient was able to open her eyes but did not track movement or follow commands. She was subsequently noted to have a left orbit that became harder to compress with ballottement test compared to the right, so Ophthalmology was consulted.
An ophthalmologic exam showed extensive chemosis of the left eye compared to the right with conjunctival hemorrhage in bilateral eyes (Figure 1).

Figure 1. Ophthalmologic exam revealed chemosis, exophthalmos, and a mid-dilated, fixed pupil of left eye compared to right.
Ocular tonometry revealed a pressure of 14 mmHg in the right eye and 53 mmHg in the left. There was a mid-dilated, fixed pupil on the left. The differential at this point included traumatic acute angle closure glaucoma versus a retroorbital process. The patient was started on timolol, pilocarpine, and dorzolamide eye drops for intraocular pressure control. An orbital CT was obtained, which showed an engorged superior ophthalmic vein on the left with a new 4 mm proptosis of the left eye (Figure 2) when compared to previous imaging.

Figure 2. A: CT scan showed proptosis of 4 mm of left eye compared to right eye. B: Enlarged left ophthalmic vein also noted on CT scan (arrow).
This raised concern for traumatic carotid cavernous fistula. A CTA obtained the following morning confirmed this suspicion (Figure 3).


Figure 3. A: Reconstructed coronal CT coronal angiogram showing enlarged left cavernous sinus, confirming diagnosis of carotid cavernous fistula. B-E: Static coronal images from CT angiogram with major arteries labeled. F: Video of CT angiogram.
The patient was transferred to an outside facility for surgical management, which consisted of angiography and embolization via coiling of her CCF.
Discussion
Carotid cavernous fistulas are abnormal connections that form between the cavernous sinus and the internal or external carotid arteries, or branches of the internal or external carotid arteries. They are divided into direct and indirect variants per Barrow classification (Table 1, Figure 4).

ICA = Internal carotid artery ECA = External carotid artery

Figure 4. A: The normal eye: superior ophthalmic vein draining into cavernous sinus and internal and external carotid arteries traversing the cavernous sinus. B: Barrow Classifications for types of carotid cavernous fistulas: Type A: direct connection between internal carotid artery and cavernous sinus. Type B: connection between dural branches of internal carotid artery and cavernous sinus. Type C: connection between dural branches of external carotid artery and cavernous sinus. Type D: connection between dural branches of both internal carotid artery and external carotid artery and the cavernous sinus.
Types B through D are commonly termed ‘indirect’ or ‘dural’ fistulas. These can develop spontaneously as a result of hypertension and are the more common presentation of CCF. More specifically, type B is a connection between the dural branches of the ICA and the cavernous sinus, type C is a connection between the dural branches of the external carotid artery (ECA) and the cavernous sinus, and type D connects the dural supply of both the ICA and ECA and the cavernous sinus (1). Type A, or a ‘direct’ CCF, is a connection between the intracavernous internal carotid artery (ICA) and the cavernous sinus. Direct CCF is a rare ocular complication that forms most commonly as a result of craniofacial trauma, but can also be due to aneurysmal rupture or spontaneous development. This is also the most dramatic presentation of CCF and was the case in our patient.
Prompt identification and management of CCF is necessary to prevent associated morbidity and mortality. The presentation of CCF depends mainly on the drainage of the fistula. Anterior-drainage of fistulas through the superior ophthalmic vein produces symptoms of exophthalmos, proptosis, acute chemosis or swelling/edema of conjunctiva, and headache, all of which are more common in direct CCFs. The backup of drainage can result in a secondary angle closure with extremely high intraocular pressure. Posterior-drainage of fistulas into the superior and inferior petrosal sinuses tend to lack the aforementioned features of orbital congestion, but can produce painful cranial neuropathy of the trigeminal, facial, or ocular motor nerves. Failure to identify and appropriately treat posterior-draining fistulas can lead to eventual reversal of flow and development of anterior drainage (4).
The signs of CCF are not visible on neuroimaging at a patient’s presentation and generally develop over the first week a patient is admitted. Clinical signs which may prompt further investigation and repeat imaging include chemosis, increasing exophthalmos, pain, and increased intraocular pressure. Often, the tools for checking intraocular pressure are not available in an ICU setting. In the absence of signs of a ruptured globe, an intensivist could palpate the orbit over a closed eye (as occurred in this case). If there is asymmetry in resistance to palpation, this should incite an ophthalmologic consult to consider a retro-orbital process.
Repeat neuroimaging is likely to be done in these cases, but it is important to order the right test. Radiologic signs of CCF include proptosis and asymmetric enlargement of a cavernous sinus or superior ophthalmic vein and would be noted on an orbital or maxillofacial CT. A head CT might miss these signs, so it is important to obtain imaging dedicated to examining the retro-orbital space. To confirm the diagnosis of CCF, one must then obtain a CT angiogram, which will show the aberrant connections between the intracranial vessels. Upon confirming a diagnosis of CCF, the preferred mode of management is endovascular obliteration using an arterial or venous approach as it has been shown to be safe and effective, and confers long-term cure in most cases (5).
A previous review of 16 cases of carotid cavernous fistulas treated with transarterial embolization with detachable balloon show satisfactory results, defined as resolution of CCF without residual disability, in 11 cases and resolution but with residual disability in 5 cases. The most common of the disabilities in these cases was vision impairment, as seen in 4 out of the 5 cases. In addition, 14 out of the 16 cases resolved with preserved internal carotid artery flow (1). As a result, transarterial embolization with detachable balloon (TAEDB) has been established as the preferred method of treatment for carotid cavernous fistulas (6). Other options for treatment include neurosurgery and stereotactic radiosurgery when endovascular approach is not feasible.
Our patient presented with several traumatic injuries following a fall down a flight of stairs and was unable to contribute to history-taking. Detection and treatment of the CCF that she later developed was complicated by several factors. The true exophthalmos of the affected eye was partially masked by the fact that she had an inferotemporal orbital fracture of the opposite eye, which was incorrectly thought to be enophthalmic. Additionally, her altered mental status and subsequent re-intubation limited her ability to vocalize the pain which would have been present in her affected eye due to tremendously increased intraocular pressure.
From a critical care physician perspective, part of the key to her diagnosis was her re-intubation. The patient developed severe agitation requiring sedation without other more typical reasons for intubation such as hypoxia, tachypnea, or dyssynchronous breathing. We suspect this agitation was likely secondary to pain from the rapidly increasing pressure in her affected eye which became symptomatic just prior to her worsening mental status. Her physical exam was ultimately crucial to the detection of her CCF, specifically chemosis, exophthalmos, and increased intraocular pressure in the affected eye. These signs led to the subsequent ophthalmologic consultation, imaging, and eventually the diagnosis of CCF.
An important lesson learned from this patient’s management is having a low threshold for consultation when the clinical picture does not match diagnostic workup. In our case, the patient’s clinical condition changed but repeat workup including EEG and MRI of the head was negative. Previous imaging had revealed right-sided facial fractures, yet her new findings, including increased resistance to palpation of the orbit and chemosis, were largely left-sided. In situations when the cause of a patient’s deteriorating condition is unclear and there is incongruity between the physical exam and diagnostic workup, it is imperative to obtain further consultation. In our case, the ophthalmic exam gave the clues for further workup and the ultimate diagnosis.
In conclusion, this patient’s case is a good study in the classic presentation of direct CCF in association with craniofacial trauma, and also illuminates the difficulty in detection of orbital injuries in a trauma patient who cannot vocalize the symptoms they are experiencing. The lesson learned from her presentation is to have a low threshold for ophthalmologic consultation for unexplained changes in ophthalmic condition and discrepancies between clinical presentation and diagnostic findings.
References
- Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985 Feb;62(2):248-56. [CrossRef] [PubMed]
- Liang W, Xiaofeng Y, Weiguo L, Wusi Q, Gang S, Xuesheng Z. Traumatic carotid cavernous fistula accompanying basilar skull fracture: a study on the incidence of traumatic carotid cavernous fistula in the patients with basilar skull fracture and the prognostic analysis about traumatic carotid cavernous fistula. J Trauma. 2007 Nov;63(5):1014-20. [CrossRef] [PubMed]
- Doran M. Carotid-Cavernous Fistulas: Prompt Diagnosis Improves Treatment. American Academy of Ophthalmology. https://www.aao.org/eyenet/article/carotid-cavernous-fistulas-prompt-diagnosis-improv. Published March 18, 2016. Accessed July 11, 2017.
- Miller NR. Diagnosis and management of dural carotid-cavernous sinus fistula. Neurosurg Focus. 2007;23(5):E13. [PubMed]
- Gupta AK, Purkayastha S, Krishnamoorthy T, Bodhey NK, Kapilamoorthy TR, Kesavadas C, Thomas B. Endovascular treatment of direct carotid cavernous fistulae: a pictorial review. Neuroradiology. 2006 Nov;48(11):831-9. [CrossRef] [PubMed]
- Lewis AI, Tomsick TA, Tew JM Jr, Lawless MA. Long-term results in direct carotid-cavernous fistulas after treatment with detachable balloons. J Neurosurg. 1996 Mar;84(3):400-4. [CrossRef] [PubMed]
Cite as: Ganapathiraju I, Summerfield DT, Summerfield MM. Carotid cavernous fistula: a case study and review. Southwest J Pulm Crit Care. 2017:15(1):32-8. doi: https://doi.org/10.13175/swjpcc083-17 PDF