
Critical Care
The Southwest Journal of Pulmonary and Critical Care publishes articles directed to those who treat patients in the ICU, CCU and SICU including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.

A Case of Brugada Phenocopy in Adrenal Insufficiency-Related Pericarditis
Andrew Kim DO
Cristian Valdez DO
Tony Alarcon MD
Elizabeth Benge MD
Blerina Asllanaj MD
MountainView Hospital
Las Vegas, NV USA
Abstract
This is a report of a 27-year-old male with known history of Addison’s disease, noncompliant with medications, and hypothyroidism who presented with shortness of breath, nausea, vomiting, fever, and chest pain as well as Brugada sign seen on electrocardiogram. Echocardiogram revealed a moderate pericardial effusion and laboratory findings were suggestive of adrenal insufficiency. Patient was determined to have Type I Brugada phenocopy, which is a Brugada sign seen on EKG with a reversible cause. In this instance, the Brugada phenocopy was caused by adrenal insufficiency with associated pericarditis. Treatment with high-dose steroids led to resolution of both the pericardial effusion and Brugada sign, providing further evidence of Brugada phenocopy.
Keywords: Brugada Phenocopy, Adrenal insufficiency, Pericarditis, Brugada Sign
Case Presentation
History of Present Illness
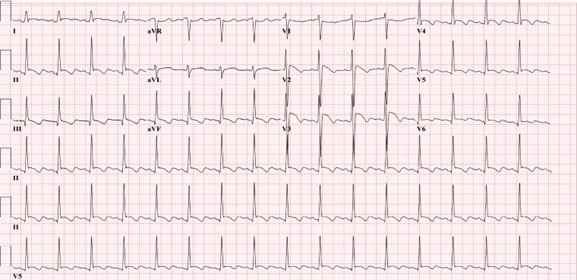
A 27-year-old man was admitted for left-sided chest pain. Electrocardiogram (EKG) taken in the emergency department showed suspicious Brugada’s sign in leads V2 and V3 (Figure 1).

Figure 1. Initial EKG showing rhythm with signs of inferior infarct based on findings of leads II, II aVL. There are also signs of anterolateral injury seen in leads V2-V5. Also, there were coved ST elevation in leads V2 and V3, suggesting a Type I Brugada sign. (Click here to open Figure 1 in an enlarged, separate window)
{kind=link}
He had been feeling short of breath, nauseous, had multiple episodes of vomiting without blood, fever of up to 102 F, and chills for five days prior to admission that had resolved. He described the pain as similar to a “pulled muscle” over his left pectoral area that was worse with extension of the left shoulder as well as with deep inhalation. He denied palpitations, diaphoresis, or radiation of the pain. He denied any family history of cardiac disease or sudden cardiac deaths. Patient lives in San Francisco and travels to Las Vegas periodically to see his family. He had been in Las Vegas for four months prior to admission. He works as a video editor from home. He denies intravenous drug use, history of sexually transmitted illnesses, or history of unsafe sexual activity.
Upon admission, his vitals were: Temp 36.2° C, BP 97/66, HR 84, respiratory rate 16, and SpO2 94% on room air. The patient was slightly hyponatremic with sodium level 131. Potassium levels were also low at 3.2. Physical exam was unremarkable with benign cardiac and respiratory findings. Chest X-ray showed small left-sided pleural effusion with surrounding area of atelectasis. The right lung was unremarkable. In light of the patient’s symptoms and abnormal EKG, an echocardiogram was planned to assess cardiac function and further lab studies were ordered.
Past Medical History
The patient was diagnosed with Addison’s disease at a young age and started on hydrocortisone 5mg daily. Patient also has a history of hypothyroidism and takes levothyroxine 50 mcg daily. Patient has a history of psoriatic arthritis and was taking methotrexate before switching to injectables. Of note, the patient states that he is noncompliant with his oral hydrocortisone 5 mg, sometimes missing multiple days at a time. He had missed three to four days of medication before symptom onset, and had been taking stress doses of 20 mg a day for five days. Given the patient’s presentation and reproducible pain with movement of the left arm, initial differentials included left pectoral strain and community acquired pneumonia. Adrenal insufficiency and autoimmune pericarditis were also considered based on the patient’s history of autoimmune disorders.
Investigation
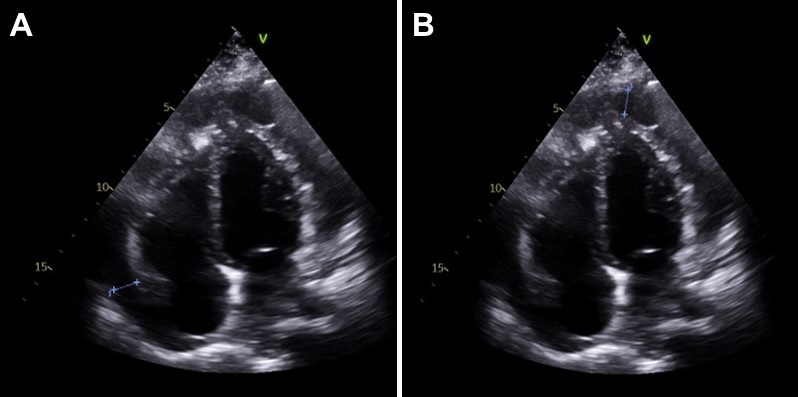
On day two of hospitalization, the patient continued to be hypotensive and febrile. Cortisol levels were found to be 1.02 mcg/dL, adrenocorticotropic hormone (ACTH) less than 1.5 ug/mL, TSH was 1.65 mcg/mL and T4 was 1.67 ng/dL. Urinalysis showed protein, a small amount of ketones, blood, nitrites, 0-2 red blood cells, 10-20 white blood cells, and 5-10 epithelial cells but was negative for leukocyte esterase and bacteria. Inpatient echocardiogram done on day two of hospitalization demonstrated a small to moderate pericardial effusion that appears complex with possible calcifications of visceral pericardium at the right ventricular apex (Figure 2).

Figure 2. Echocardiogram. A: shows a pericardial effusion lateral to the left atrium, 1.20 centimeters in diameter. B: shows a pericardial effusion at the apex of the right ventricle, 1.24 centimeters in diameter. (Click here to open Figure 2 in an enlarged, separate window)
{kind=link}
Immunologic work-up was also completed and demonstrated high complement C3 at 187 mg/dL. Viral work-up was also negative. Further investigation of history revealed that the patient had experienced similar symptoms in the past - shortness of breath, fever, nausea - especially during stressful times in his life, but attributed it to anxiety.
Management
Patient was immediately started on intravenous hydrocortisone 50mg every 6 hours after cortisol labs were returned, with the plan to wean to twice a day on the next day and then switching to oral hydrocortisone 20 mg daily. The patient was also started on ceftriaxone 1 gram daily for possible urinary tract infection and doxycycline 100mg twice a day. He complained of dizziness and weakness after switching to oral hydrocortisone, and the dosage was increased to 25 mg daily. The patient stated that after the increase in steroids these symptoms resolved and he had increased energy. His blood pressure remained stable with no episodes of hypotension after switching to oral steroids and his electrolyte panel remained within normal limits.
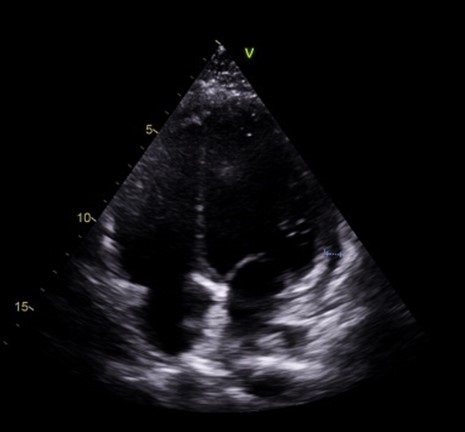
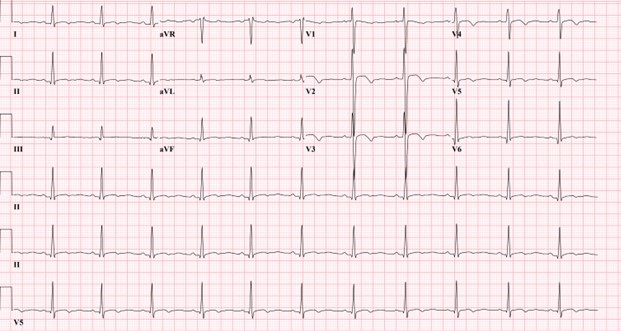
Follow-up echocardiogram on day five of hospital stay demonstrated a trivial pericardial effusion that had decreased significantly in comparison to the previous study (Figure 3). Repeat electrocardiogram demonstrated normal sinus rhythm with no Brugada sign (Figure 4).

Figure 3. Slight pericardial effusion lateral to the right ventricle, 0.6 centimeters in diameter. Note that there is marked decrease in fluid along the left atrium and apex of the right ventricle compared to Figure 2. (Click here to open Figure 3 in an enlarged, separate window)
{kind=link}

Figure 4. Electrocardiogram taken after steroid treatment prior to discharge. Normal sinus rhythm seen in results. Also note normalization in leads V2 and V3 with no clear Brugada seen. (Click here to open Figure 4 in an enlarged, separate window)
{kind=link}
Discussion
Our patient’s presentation of shortness of breath, nausea, vomiting, fever, and chest pain with negative viral work-up is suggestive of early stages of adrenal insufficiency crisis. Our diagnosis is further evidenced by the patient’s noncompliance with his home steroid doses as well as a morning cortisol level of 1.02 mcg/dL and ACTH less than 1.5 ug/mL. There have been reported cases of adrenal insufficiency causing Type I Brugada phenocopy and normalization with treatment (1). The normalization of our patient’s EKG and pericarditis after treatment with high dose steroids is evidence of Brugada phenocopy in this case. In addition, pericarditis has been shown to present as a Type 1 Brugada phenocopy (BrP), a Brugada sign seen on EKG with a reversible cause (2).
One common cause of BrP is electrolyte abnormalities, as BrP can be seen in patients with profound hyponatremia and hyperkalemia (3,4). In particular, hyperkalemia is a common culprit of Brugada sign on EKG as potassium excess can decrease the resting membrane potential (5). Typically, patients with adrenal insufficiency will exhibit electrolyte abnormalities that can explain Brugada sign on EKG. This patient’s electrolytes were indicative of hyponatremia and hypokalemia upon presentation. Although the electrolyte abnormalities were mild, the hyponatremia in particular contributed to the team’s initial suspicion of adrenal insufficiency. To our knowledge, this is the first instance of Brugada sign and pericarditis seen together in adrenal insufficiency crisis. Cases of Brugada pattern in adrenal crisis have been reported (6), however no echocardiogram was done in these case reports.
In addition, reported cases of pericarditis caused by Brugada phenocopy offers an alternative view of the sequence of events in this patient (7). Pericardial disease is known to cause Brugada phenocopy, and this may have been the case in our patient. Both pericarditis and BrP can be caused by adrenal insufficiency, so it is also possible that both of these events were independent of each other and stem from the underlying adrenal insufficiency. As such, this case highlights an important point mentioned in the previous case reports: the need to consider both pericarditis and adrenal insufficiency crisis in a patient presenting with Brugada phenocopy.
Conclusion
In conclusion, in patients presenting with Brugada sign the possibility of adrenal insufficiency crisis as well as pericarditis should be considered, especially in patients with known Addison’s disease. Furthermore, patients presenting with Brugada sign with no history of genetic cardiac history or family history of sudden cardiac death should be evaluated for other causes, such as adrenal insufficiency or pericarditis.
References
- Anselm DD, Evans JM, Baranchuk A. Brugada phenocopy: A new electrocardiogram phenomenon. World J Cardiol. 2014 Mar 26;6(3):81-6. [CrossRef] [PubMed]
- Monti M, Olivi G, Francavilla F, Borgognoni F. Pericarditis mimicking Brugada syndrome. Am J Emerg Med. 2017 Apr;35(4):669.e1-669.e3. [CrossRef] [PubMed]
- Hunuk A, Hunuk B, Kusken O, Onur OE. Brugada Phenocopy Induced by Electrolyte Disorder: A Transient Electrocardiographic Sign. Ann Noninvasive Electrocardiol. 2016 Jul;21(4):429-32. [CrossRef] [PubMed]
- Manthri S, Bandaru S, Ibrahim A, Mamillapalli CK. Acute Pericarditis as a Presentation of Adrenal Insufficiency. Cureus. 2018 Apr 13;10(4):e2474. [CrossRef] [PubMed]
- Yan GX, Antzelevitch C. Cellular basis for the Brugada syndrome and other mechanisms of arrhythmogenesis associated with ST-segment elevation. Circulation. 1999 Oct 12;100(15):1660-6. [CrossRef] [PubMed]
- Iorgoveanu C, Zaghloul A, Desai A, Balakumaran K, Adeel MY. A Case of Brugada Pattern Associated with Adrenal Insufficiency. Cureus. 2018 Jun 6;10(6):e2752. [CrossRef] [PubMed]
- Shehadeh M, O'Donoghue S. Acute Pericarditis-Induced Brugada Phenocopy: A Case Report and Review of the Literature. Cureus. 2020 Aug 15;12(8):e9761. [CrossRef] [PubMed]
Cite as: Kim A, Valdez C, Alarcon T, Benge E, Asllanaj B. A Case of Brugada Phenocopy in Adrenal Insufficiency-Related Pericarditis. Southwest J Pulm Crit Care Sleep. 2022;25(2):25-29. doi: https://doi.org/10.13175/swjpccs033-22 PDF
Ultrasound for Critical Care Physicians: Sometimes It’s Better to Be Lucky than Smart
Robert A. Raschke MD and Randy Weisman MD
Critical Care Medicine
HonorHealth Scottsdale Osborn Medical Center
Scottsdale, AZ USA
We recently responded to a code arrest alert in the rehabilitation ward of our hospital. The patient was a 47-year-old man who experienced nausea and diaphoresis during physical therapy. Shortly after the therapists helped him sit down in bed, he became unconsciousness and pulseless. The initial code rhythm was a narrow-complex pulseless electrical activity (PEA). He was intubated, received three rounds of epinephrine during approximately 10 minutes of ACLS/CPR before return of spontaneous circulation (ROSC), and was subsequently transferred to the ICU.
Shortly after arriving, a 12-lead EKG was performed (Figure 1), and PEA recurred.

Figure 1. EKG performed just prior to second cardiopulmonary arrest showing S1 Q3 T3 pattern (arrows).
Approximately ten-minutes into this second episode of ACLS, a cardiology consultant informed the code team of an S1,Q3,T3 pattern on the EKG. A point-of-care (POC) echocardiogram performed during rhythm checks was technically-limited, but showed a dilated hypokinetic right ventricle (see video 1).

Video 1. Echocardiogram performed during ACLS rhythm check: Four-chamber view is poor quality, but shows massive RV dilation and systolic dysfunction.
Approximately twenty-minutes into the arrest, 50mg tissue plasminogen activator (tPA) was administered, and return of spontaneous circulation (ROSC) achieved two minutes later. A tPA infusion was started. The patient’s chart was reviewed. He had received care in our ICU previously, but this wasn’t immediately recognized because he had subsequently changed his name of record to the pseudonym “John Doe” (not the real pseduonym), creating two separate and distinct EMR records for the single current hospital stay. Review of the first of these two records, identified by his legal name, revealed he had been admitted to our ICU one month previously for a 5.4 x 3.6 x 2.9 cm left basal ganglia hemorrhage. We stopped the tPA infusion.
On further review of his original EMR is was noted that two weeks after admission for intracranial hemorrhage, (and two weeks prior to cardiopulmonary arrest), he had experienced right leg swelling and an ultrasound demonstrated extensive DVT of the right superficial femoral, saphenous, popliteal and peroneal veins. An IVC filter had been due to anticoagulant contraindication. The patient’s subsequent rehabilitation had been progressing well over the subsequent two weeks and discharge was being discussed on the day cardiopulmonary arrest occurred.
On post-arrest neurological examination, the patient gave a left-sided, thumbs-up to verbal request. Ongoing hypotension was treated with a norepinephrine infusion and inhaled epoprostenol. An emergent head CT was performed and compared to a head CT from four weeks previously (Figure 2), showing normal evolution of the previous intracranial hemorrhage without any new bleeding.

Figure 2. CT brain four weeks prior to (Panel A), and immediately after cardiopulmonary arrest and administration of tPA (Panel B), showing substantial resolution of the previous intracranial hemorrhage.
A therapeutic-dose heparin infusion was started. An official echo confirmed the findings of our POC echo performed during the code, with the additional finding of McConnell’s sign. McConnell’s sign is a distinct echocardiographic finding described in patients with acute pulmonary embolism with regional pattern of right ventricular dysfunction, with akinesia of the mid free wall but normal motion at the apex (1). A CT angiogram showed bilateral pulmonary emboli, and interventional radiology performed bilateral thrombectomies. Hypotension resolved immediately thereafter. The patient was transferred out of the ICU a few days later and resumed his rehabilitation.
A few points of interest:
- IVC filters do not absolutely prevent life-threatening pulmonary embolism (2,3).
- Sometimes, serendipity smiles, as when the cardiologist happened into the room during the code, and provided an essential bit of information.
- Emergent POC ultrasonography is an essential tool in the management of PEA arrest of uncertain etiology.
- Barriers to access of prior medical records can lead to poorly-informed decisions. But in this case, ignorance likely helped us make the right decision.
- Giving lytic therapy one month after an intracranial hemorrhage is not absolutely contra-indicated when in dire need.
- As the late great intensivist, Jay Blum MD used to say: “Sometimes it’s better to be lucky than smart.”
References
- Ogbonnah U, Tawil I, Wray TC, Boivin M. Ultrasound for critical care physicians: Caught in the act. Southwest J Pulm Crit Care. 2018;17(1):36-8. [CrossRef]
-
Urban MK, Jules-Elysee K, MacKenzie CR. Pulmonary embolism after IVC filter. HSS J. 2008 Feb;4(1):74-5. [CrossRef] [PubMed]
-
PREPIC Study Group. Eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC (Prevention du Risque d'Embolie Pulmonaire par Interruption Cave) randomized study. Circulation. 2005 Jul 19;112(3):416-22. doi: [CrossRef] [PubMed]
Cite as: Raschke RA, Weisman R. Ultrasound for Critical Care Physicians: Sometimes It’s Better to Be Lucky than Smart. Southwest J Pulm Crit Care. 2021;22(6):116-8. doi: https://doi.org/10.13175/swjpcc016-21 PDF
Severe Accidental Hypothermia in Phoenix? Active Rewarming Using Thoracic Lavage
Michael Mozer BS1
Guy Raz, MD2
Ryan Wyatt, MD2
Alexander Toledo, DO, PharmD2
1University of New England College of Osteopathic Medicine
Biddeford, ME USA
2Department of Emergency Medicine
Maricopa Medical Center, Phoenix, AZ USA
Abstract
Hypothermia can progress quickly and become life threatening if left untreated. Rewarming in the severely hypothermic patient is of critical importance and is achieved with active and passive techniques. Here we present a case of a hypothermic patient with cardiac instability for whom thoracic lavage was ultimately used. We will review the treatment of hypothermia and discuss the technical aspects our approach.
Case Presentation
A 53 year-old male with a past medical history of substance abuse, chronic hepatitis C, and poorly controlled type 2 diabetes mellitus complicated by a recent hospitalization for osteomyelitis was brought to the emergency department after being found lying on a road in a shallow pool of water in the early morning hours of a rainy day in Phoenix, Arizona. The ambient temperature that night was 39 °F (3.9 °C). Emergency Medical Services (EMS) noted a decreased level of consciousness and obtained a finger stick glucose of 15 mg/dl. EMS reported a tympanic membrane temperature of 23.9 °C. En route, the patient was administered 2mg naloxone and 25g dextrose intravenously with no improvement in his mental status. On Emergency Department (ED) arrival, the patient had a GCS of 8 (Eyes 4, Verbal 1, Motor 3) and exhibited intermittent posturing. His foot wound appeared clean and without signs of infection. The initial core temperature recorded was 25.9°C via bladder thermometer, systolic blood pressure was 92/50, and heart rate fluctuated between 50 and 90 beats per minute.
After removing wet clothing, initiation of warmed saline, and placing a forced warm air blanket on the patient, he was intubated for airway protection and vasopressors were initiated. Osborn waves were evident on the initial EKG (Figure 1).

Figure 1. Initial EKG with Osborn Waves (arrows).
A warmed ventilator circuit was initiated with only 0.5 °C increase in temperature in first 30 minutes. Despite these measures, he remained hypotensive and unstable. Significant laboratory findings were a white blood cell count of 25.5 thousand (92% neutrophils), lactic acid of 7.6, potassium of 5.8, serum creatinine of 1.05, glucose of 283, INR of 1.1, and urine drug screen positive for cocaine. Given his recalcitrance to norepinephrine and risk of death secondary to fatal dysrhythmia with temperatures below 28 °C intrathoracic lavage initiated.
The right hemithorax was selected for irrigation because left-sided tube placement can induce ventricular fibrillation in a perfusing patient (1). Using standard sterile technique, two 36 French thoracostomy tubes were placed; the first in the second intercostal space along the mid-clavicular line, and the second in the 5th intercostal space in the posterior axillary line (1-3). The tips of the thoracostomy tubes were oriented such that the anterior-superior tube was positioned near the right apex and the lateral-inferior tip was positioned low in the thoracic cavity (1,3). To maintain the temperature of the instilled fluid, a fluid warmer system (Level 1; Smiths Medical; Minneapolis, MN) was used and set to 41 °C. A Christmas tree adapter was used to connect the IV tubing to the superior thoracostomy tube, and a water seal chamber was attached to the inferior tube for passive drainage (3). Flow through the system was targeted to maintain steady passive drainage as described in the literature (1-6).
Thoracic cavity lavage with 41 °C saline was performed and the patient was transferred to the medical ICU after 3 hours in the ED. When he was transferred his core temperature was 29 °C and he remained on norepinephrine for hemodynamic instability. After 2 hours of continued rewarming in the MICU, his core temperature was 32 °C. Osborn waves evident on initial EKG were resolved (Figure 2).

Figure 2. Repeat EKG showing resolution of Osborn waves.
The patient left against medical advice from the hospital 4 days later neurologically intact and without sequela.
Discussion
Hypothermia can be clinically classified as mild, moderate or severe (7). Mild hypothermia, defined as core temperatures of 32-35 °C, presents with shivering. Amnesia, dysarthria, ataxia, tachycardia, and tachypnea can also be seen (1). Moderate hypothermia, defined as core temperatures of 28-32 °C, usually can present with or without shivering. Stupor, hypoventilation, paradoxical undressing and non-fatal arrhythmias such as atrial fibrillation and junctional bradycardia may also be seen (1). Patients with severe hypothermia, generally defined as temperatures below 28 °C, can present with coma, areflexia, pulmonary edema, bradycardia, and hypotension (1). There is a significant risk of fatal cardiac dysrhythmias without rapid therapeutic rewarming (1,7,8).
Rewarming in the hypothermic patient is of critical importance and is achieved with passive and/or active techniques. Attempts to limit heat loss are often unsuccessful, especially in the absence of a normal shiver response. It however remains as the first line treatment for hypothermia (8-10). Passive rewarming is attempted by the removal of cold/wet clothing and keeping the patient covered (8-10). Active external rewarming (AER) is the next line of treatment and consist of the use of externally rewarming devices such as warmed blankets, warm environment, forced air warming (Bair Hugger; 3M; Maplewood, MN) or warm hot water bladders placed in the groin and axilla (1,7-10). Active Internal Rewarming (AIR) techniques can be used to achieve more rapid increases in core temperature and are primarily utilized in cases of cardiac instability or if AER is unsuccessful (8). When available, the method of choice for active internal rewarming (AIR) is cardiopulmonary bypass (CPB) or extracorporeal membrane oxygenation (ECMO) as they can achieve the fastest increase in core temperature (9 °C/hr and 6 °C/hr respectively) and provide cardiovascular support (1,8,11,12). Several techniques are described in the literature that can be considered if CPB or ECMO are unavailable. These include esophageal warming devices, endovascular catheters, hemodialysis, and endocavitary lavage (1,2,4-6,13-15). While no randomized controlled trials exist, several case reports and reviews have tried to compare various techniques. These sources to do not seem to favor any particular technique over another but rather reports the rates of temperature rise (1-3,5-7,13-15). Classically, lavage techniques are attempted in the thoracic cavity, the peritoneum, the bladder, the stomach, the esophagus, or the colon. These techniques are generally coupled with warm IV fluids and warming air through the ventilator to limit loss of body heat to iatrogenic procedures during the rewarming attempt (1,7). Thoracic lavage is effective with a reported rewarming rates of 3-6 °C/hr and with excellent outcomes in case reports (1,2,4-6). Here we present a case of a hypothermic patient with cardiac instability where thoracic lavage is used and discuss the technical aspects of this approach.
Our case demonstrates the efficacy of utilizing thoracic cavity lavage for rapid rewarming in patients with severe hypothermia with a pulse and at high risk of fatal cardiac arrhythmia. In multiple case reports, thoracic lavage has been used successfully in hypothermic patients who suffered complete cardiopulmonary collapse requiring CPR (2,4,5). Although warm thoracic lavage is not the treatment of choice in these circumstances, in a facility not equipped with ECMO or CPB and a patient too unstable to transfer, it seemed to us to be the best technique. Gastric, colonic, and bladder lavage offer very minimal heat transfer due to limitations in surface area (2).
Hemodialysis would have required for us to call in a technician and would have required approval by a nephrologist at our institution. Available central venous rewarming catheters require bypass of a failsafe mechanism that does not allow rewarming to be initiated below 30 °C (1). Peritoneal lavage was a plausible choice but does not directly warm the mediastinum (2). While an open mediastinal technique has been used, we did not feel it was appropriate in a patient with a concurrent pulse (1,3). Thoracic lavage is therefore an effective alternative that should be used in cases where CPB and ECMO are unavailable especially in a patient that is hemodynamically unstable and may not survive transfer. The equipment is readily available to any Emergency Medicine or Critical Care physician. In addition, this case exemplifies the positive outcomes that are associated with rapid rewarming in the hypothermic patient with a pulse. We believe our case demonstrates the efficacy of this technique for myocardial protection from hemodynamic collapse, a topic which has not been adequately studied in the literature.
References
- Brown DJ, Danzl DF. Accidental hypothermia. In: Auerbach PS, ed. Wilderness Medicine. 7th ed. St. Louis: Mosby Inc.; 2017:135-62.
- Plaisier BR. Thoracic lavage in accidental hypothermia with cardiac arrest--report of a case and review of the literature. Resuscitation. 2005 ;66(1):99-104. [CrossRef] [PubMed]
- Schiebout JD. Hypothermic Patient Management. In: Reichman EF. eds. Reichman's Emergency Medicine Procedures, 3e New York, NY: McGraw-Hill. Available at: http://accessemergencymedicine.mhmedical.com/content.aspx?bookid=2498§ionid=201303754 (accessed August 02, 2019).
- Little G. Accidental hypothermic cardiac arrest and rapid mediastinal warming with pleural lavage: A survivor after 3.5 hours of manual CPR. BMJ Case Reports. July 2017:bcr-2017-220900. [CrossRef] [PubMed]
- Turtiainen J, Halonen J, Syväoja S, Hakala T. Rewarming a patient with accidental hypothermia and cardiac arrest using thoracic lavage. Ann Thorac Surg. 2014 Jun;97(6):2165-6. [CrossRef] [PubMed]
- Ellis MM, Welch RD. Severe hypothermia and cardiac arrest successfully treated without external mechanical circulatory support. Am J Emerg Med. 2016;34(9):1913.e5-6. [CrossRef] [PubMed]
- Tintinalli J, Stapczynski J, Ma O, Yealy D, Meckler G, Cline D. Tintinalli's Emergency Medicine. 8th ed. New York, NY: McGraw-Hill Education; 2016:1743-4.
- Brugger H, Boyd J, Paal P. Accidental Hypothermia. N Engl J Med. 2012;367(20):1930-8. [CrossRef] [PubMed]
- Paal P, Gordon L, Strapazzon G, et al. Accidental hypothermia-an update: The content of this review is endorsed by the International Commission for Mountain Emergency Medicine (ICAR MEDCOM). Scand J Trauma Resusc Emerg Med. 2016;24(1):111. [CrossRef] [PubMed]
- Zafren K, Giesbrecht GG, Danzl DF, et al. Wilderness Medical Society practice guidelines for the out-of-hospital evaluation and treatment of accidental hypothermia: 2014 update. Wilderness Environ Med. 2014 Dec;25(4 Suppl):S66-85. [CrossRef] [PubMed]
- Schober A, Sterz F, Handler C, et al. Cardiac arrest due to accidental hypothermia-A 20 year review of a rare condition in an urban area. Resuscitation. 2014;85(6):749-56. [CrossRef] [PubMed]
- Saczkowski RS, Brown DJA, Abu-Laban RB, Fradet G, Schulze CJ, Kuzak ND. Prediction and risk stratification of survival in accidental hypothermia requiring extracorporeal life support: An individual patient data meta-analysis. Resuscitation. 2018;127:51-7.[CrossRef] [PubMed]
- Primozic KK, Svensek F, Markota A, Sinkovic A. Rewarming after severe accidental hypothermia using the esophageal heat transfer device: a case report. Ther Hypothermia Temp Manag. 2018 Mar;8(1):62-4. [CrossRef] [PubMed]
- Murakami T, Yoshida T, Kurokochi A, et al. Accidental hypothermia treated by hemodialysis in the acute phase: three case reports and a review of the literature. Intern Med. 2019 Jun 7. [CrossRef]
- Klein LR, Huelster J, Adil U, et al. Endovascular rewarming in the emergency department for moderate to severe accidental hypothermia. Am J Emerg Med. 2017 Nov;35(11):1624-9. [CrossRef] [PubMed]
Cite as: Mozer M, Raz G, Wyatt R, Toledo A. Severe accidental hypothermia in Phoenix? Active rewarming using thoracic lavage. Southwest J Pulm Crit Care. 2019;19(2):79-83. doi: https://doi.org/10.13175/swjpcc038-19 PDF
January 2019 Critical Care Case of the Month: A 32-Year-Old Woman with Cardiac Arrest
Sarah A. Watkins, DO1
Geoffrey Smelski, PharmD1
Robert N.E. French, MD1
Michael Insel, MD2
Janet Campion MD2
1Arizona Poison and Drug Information Center and 2Division of Pulmonary, Allergy, Critical Care and Sleep
University of Arizona
Tucson, AZ USA
History of Present Illness
A 32-year-old woman with history of chronic neck pain and opioid abuse complained of dizziness and palpitations shortly before suffering a witnessed cardiac arrest in her home. She was given bystander cardiopulmonary resuscitation until emergency medical services arrived on scene, at which point intermittent polymorphic ventricular tachycardia with a pulse was noted on the cardiac monitor and physical exam (Figure 1).

Figure 1. Rhythm strips showing ventricular tachycardia (A) and a prolonged QT interval (B).
Which of the following is (are) the most likely cause(s) of the cardiac arrythmia? (Click on the correct answer to be directed to the second of seven pages)
Cite as: Watkins SA, Smelski G, French RNE, Insel M, Campion J. January 2019 critical care case of the month: A 32-year-old woman with cardiac arrest. Southwest J Pulm Crit Care. 2019;18(1):1-7. doi: https://doi.org/10.13175/swjpcc121-18 PDF